
Tommy John Injury: Journey Back to Throwing after a UCL Injury
archivado en Tratos
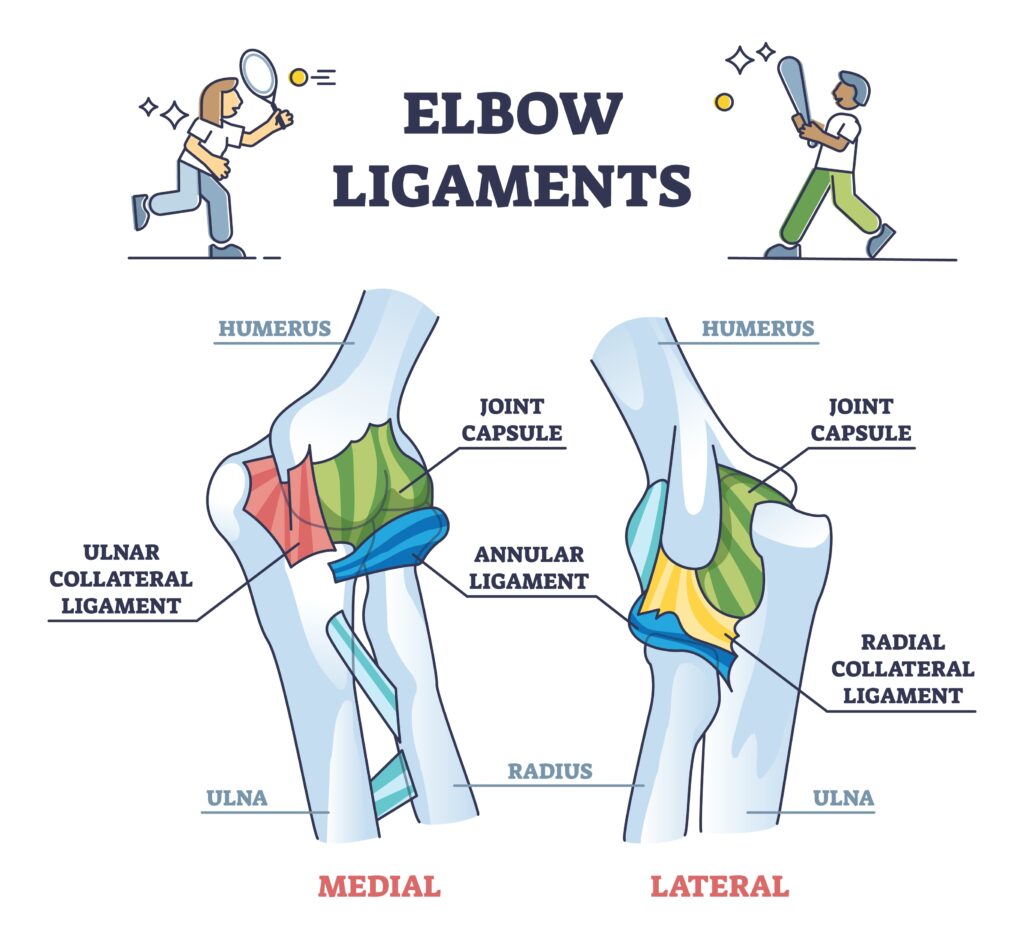
Anatomy of Ulnar Collateral Ligament (UCL)
Originating on the anteroinferior surface of the medial epicondyle of the humerus and inserting onto the sublime tubercle of the ulna, the ulnar collateral ligament (UCL), also known as the medial collateral ligament (MCL), is crucial in providing support to the medial aspect of the codo by restraining valgus instability, especially during overhead throwing motions (Labott et al., 2018). The UCL has three bundles: anterior, posterior, and transverse. Since the anterior bundle is the primary stabilizer of valgus stress which occurs the most during overhead throwing motions, that specific bundle of the UCL is injured most commonly in throwers who suffer a Tommy John injury (Paci, 2024).
What is a Tommy John Injury?
A Tommy John injury occurs when someone stretches or tears their UCL located on the medial side of their codo (Cleveland Clinic, 2025). This injury can be caused by a sudden acute injury, but it is primarily due to overuse, which is why it is so common in athletes that perform repetitive strenuous overhead movements, like baseball pitchers. In fact, Tommy John is the name of a baseball pitcher who suffered from a severe tear of his ulnar collateral ligament.
What are the Symptoms of a Tommy John Injury?
Tommy John injuries have three levels of severity: grade one indicates the ligament is stretched but not torn, grade two indicates the ligament is partially torn, and grade three indicates the ligament is completely torn (Cleveland Clinic, 2025). If someone has a mild or moderate UCL injury (grade one or two), then they can experience the following symptoms:
- weakness with overhead movements
- pain and tenderness on the medial side of their affected codo when performing overhead movements and/or sudden jerky movements
- instability in the affected codo, and/or
- weaker grip strength of the hand of the affected upper extremity.
If someone has a severe UCL injury (grade three), then they can experience the following symptoms:
- a sudden pop in the affected codo likely when the ligament tore
- severe pain in the affected codo
- inability to do overhead movements like throwing, and/or
- numbness/tingling in the ring and pinky fingers of the affected upper extremity.
What Does Treatment After Surgical Intervention Look Like?
Depending on how severe the injury is, treatment can be non-surgical or surgical. Surgical interventions for a completely torn UCL is a UCL reconstruction surgery, which involves replacing the injured ligament with a new tendon harvested from another part of the body or from a donor’s body (John Hopkins Medicine, n.d.). To get a thrower back to playing competitively, the recovery timeline can be as quick as 9 months, but, more typically, it is around 12-18 months long (Kinetic Sports Medicine & Performance, 2023). There are many factors that affect the recovery timeline; for example, timelines can differ depending on the position a person plays in their sport or simply from the fact that people’s bodies heal differently from others. During the post-op rehabilitation process, there are multiple phases of an individual’s recovery with different goals to ensure proper healing of the graft. According to Massachusetts General Hospital Sports Medicine, a standard treatment timeline for a UCL reconstruction surgery can look like the following:
- Immediate Post-Op Phase (weeks 0-3)
- Focus: protect tendon reconstruction and surgical site, manage pain and inflammation, and decrease muscle atrophy
- Patient’s codo is immobilized in a splint or brace for this period of time.
- Protection Phase (weeks 4-6)
- Focus: promote healing of repaired tissues, gradually increase to full range of motion (ROM) by week 6, slowly integrate exercises to help regain muscular strength, and restore full function of graft site.
- At week 6, patient’s codo splint or brace can be discharged if there are no complications. Also, gentle strengthening exercises and the Thrower’s Ten Program can be introduced at this time.
- Strengthening Phase (weeks 6-12)
- Focus: increase strength, power, and endurance and maintain full ROM of codo
- At week 8, patient can progress to the advanced portion of the Thrower’s Ten Program if there are no complications.
- Advanced Strengthening Phase (weeks 12-16)
- Focus: keep progressing power and endurance and normalize affected upper extremity’s strength
- Return to Activity or Sport Phase (weeks 16+)
- Focus: increase strength, power, and endurance, safely introduce sport specific training program, and safely progress patient fully back into their sport
What is the Thrower’s Ten Program?
The Thrower’s Ten Program is an exercise program, specifically for overhead throwing athletes like baseball pitchers, that is implemented into the post-op rehab journey after ROM is regained to help restore strength, stability, coordination, and endurance of the shoulder and codo muscles while incorporating proper throwing mechanics (Gokalp & Kirmizigil, 2020). It is a program that bridges basic therapy exercises to sport-specific training, allowing these athletes to effectively return to their sport’s specific activities and begin interval throwing safely after surgery.
Referencias
Cleveland Clinic. (2025, June 19). UCL (Tommy John) injury: What it is, symptoms & treatment. Cleveland Clinic. https://my.clevelandclinic.org/health/diseases/22760-ulnar-collateral-ligament-ucl-injuries
Gokalp, O., & Kirmizigil, B. (2020). Effects of Thrower’s Ten exercises on upper extremity performance: A randomized controlled study. Medicine, 99(42), e22837. https://doi.org/10.1097/MD.0000000000022837
Johns Hopkins Medicine. (n.d.). Tommy John Surgery (Ulnar Collateral Ligament Reconstruction). Retrieved November 26, 2025, from https://www.hopkinsmedicine.org/health/treatment-tests-and-therapies/tommy-john-surgery-ulnar-collateral-ligament-reconstruction
Kinetic Sports Medicine & Performance. (2023, March 1). Tommy John Injury (The Complete Guide). Kinetic Sports Medicine & Performance. https://kineticsmp.com/blog/tommy-john-injury-the-complete-guide
Labott, J. R., Woo, S. L.-Y., & Glousman, R. (2018). Understanding the medial ulnar collateral ligament of the elbow. PMC. https://pmc.ncbi.nlm.nih.gov/articles/PMC6033709/
Massachusetts General Hospital Sports Medicine. (2018, November). Rehabilitation protocol for ulnar collateral ligament reconstruction (Palmaris Longus graft, Gracilis graft). https://www.massgeneral.org/assets/mgh/pdf/orthopaedics/sports-medicine/physical-therapy/rehabilitation-protocol-for-ucl-reconstruction-gracilis-graft.pdf
Paci, J. M. (2024, August 12). Tommy John surgery: Medial/ulnar collateral ligament (UCL) injury & reconstruction. SportsMD.
Más para leer

Revisión del artículo: ¿Movimiento relativo para la reparación del tendón extensor en la zona V-VI? ¿Es beneficiosa una órtesis de mano en reposo nocturno?
Hirth, MJ, Hunt, I., Briody, K., Milner, Z., Sleep, K., Chu, A., Donovan, E. y O'Brien, L. (2021). Comparación de dos programas ortopédicos de extensión de movimiento relativo después de la reparación quirúrgica de los tendones extensores de los dedos en las zonas V-VI: un ensayo de equivalencia aleatorio. Journal of Hand Therapy: por publicarse. The Skinny: Después de una reparación del tendón de la zona V-VI,…

Comparación de las tasas de recuperación entre cuatro cirugías de hombro comunes
Revisión rápida de: Case Peters Comparación de las tasas de recuperación entre cuatro cirugías de hombro comunes Grubhofer, F., Martinez, ARM, Ernstbrunner, L., Haberli, J., Selig, ME y Warner, JJ (2021) Velocidad de recuperación de las cirugías de hombro más comunes realizadas. JSES Internacional.5(4); 776-781. doi: 10.1016/j.jseint.2021.03.007 The Skinny: Establecer expectativas realistas para la trayectoria de recuperación es…

Aspectos destacados de la cirugía y la terapia de la mano para la enfermedad de Dupuytren
La enfermedad de Dupuytren afecta la fascia de la mano (mano con fasciectomía de Dupuytren). Es relativamente común encontrarse con pacientes con la enfermedad de Dupuytren, incluso si esa no es la razón principal por la que se trata al paciente. Los pacientes a menudo presentan nódulos en la palma de la mano, o incluso pueden tener un cordón engrosado...

Un ensayo clínico aleatorizado que compara programas de movimiento activo temprano: función temprana de la mano, TAM y satisfacción ortopédica con un programa de extensión de movimiento relativo para reparaciones del tendón extensor de las zonas V y VI
Por Brittany Day Collocott SJ, Kelly E, Foster M, Myhr H, Wang A, Ellis RF. Un ensayo clínico aleatorizado que compara programas de movimiento activo temprano: función temprana de la mano, TAM y satisfacción ortopédica con un programa de extensión de movimiento relativo para reparaciones del tendón extensor de las zonas V y VI. Revista de terapia de manos. 2019. doi:10.1016/j.jht.2018.10.003 El Flaco- Esto es…

¡Regístrese para recibir actualizaciones directamente en su bandeja de entrada!
Regístrese con nosotros y le enviaremos publicaciones periódicas en el blog sobre todo lo relacionado con la terapia de manos, avisos cada vez que subamos nuevos videos y tutoriales, junto con folletos, protocolos y otra información útil.