
鉴别诊断:扳机指 vs. 半脱位矢状带损伤 vs. 半脱位侧带损伤
Hand therapists frequently encounter patients presenting with finger pain, clicking, and difficulty with tendon glide. Among the most commonly confused conditions are 扳机 手指, 半脱位 sagittal band injury, and 半脱位 lateral band. Each of these pathologies involves different anatomical structures and biomechanical disruptions, but their overlapping clinical features can complicate accurate diagnosis. Understanding the subtle differences in presentation and performing targeted physical exams are crucial for appropriate treatment planning.
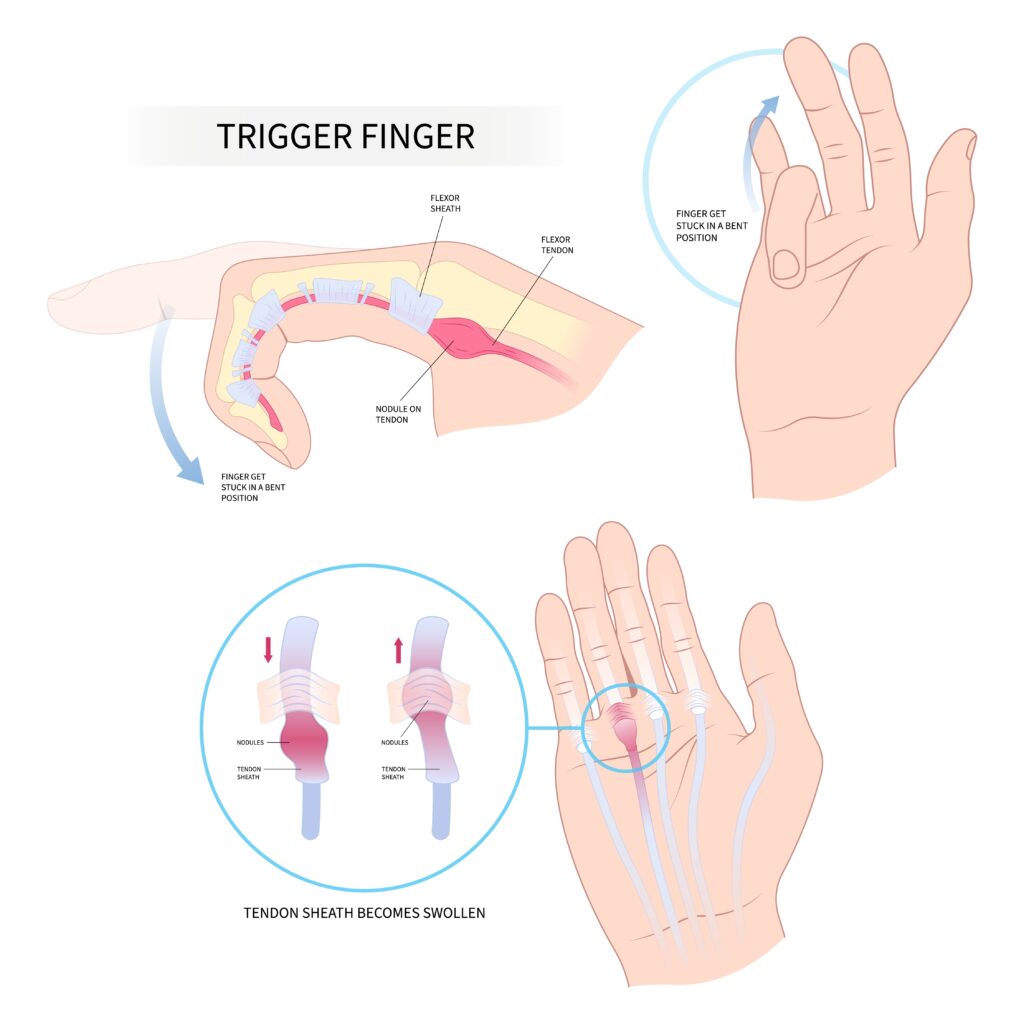
扣扳机的手指 or stenosing tenosynovitis, is a condition in which the flexor tendon becomes entrapped at the A1 pulley, typically due to thickening or inflammation of the tendon or pulley system. Patients often report a painful catching or locking sensation at the level of the metacarpophalangeal (MCP) joint, most commonly in the middle or ring fingers. On examination, passive flexion is typically smooth, but active extension may be met with resistance, followed by a sudden release, hence the “扳机” effect (Makkouk et al., 2008). Palpation often reveals a tender nodule at the volar MCP crease.
Subluxing Sagittal Band Injury, frequently referred to as “Boxer’s Knuckle,” occurs when the sagittal band fails to stabilize the extensor tendon over the MCP joint. This condition is most commonly seen in the long finger due to its increased excursion and susceptibility to trauma. Clinically, patients may report snapping or shifting of the extensor tendon during MCP flexion and extension. The hallmark physical exam finding is visible or palpable ulnar subluxation of the extensor tendon when the MCP is flexed and extended with resistance (Rayan & Young, 2006). Pain is typically localized dorsally over the MCP joint, and swelling may be present.
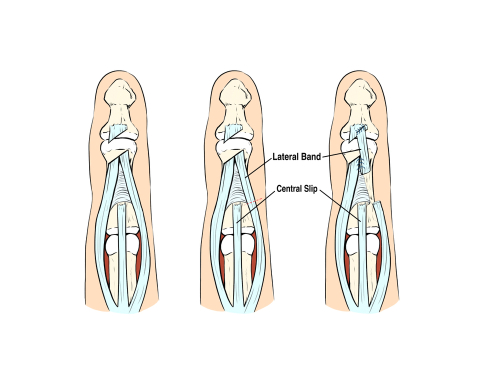
Subluxing Lateral Band injuries are less common and often occur in patients with connective tissue disorders (e.g., rheumatoid arthritis) or following trauma. The lateral bands, which contribute to PIP extension, may sublux volarly or dorsally due to rupture or laxity in the transverse retinacular ligaments. When subluxed volarly, the lateral bands may act as flexors of the PIP joint rather than extensors, mimicking boutonnière deformity. On exam, therapists may notice PIP flexion with DIP hyperextension and observe lateral band movement on active PIP flexion/extension. Palpation may detect band instability during resisted PIP movements (Harris & Rutledge, 2016).
These conditions are often confused because they can all present with clicking, pain near the MCP joint, and dysfunction during tendon excursion. For example, a 半脱位 sagittal band may mimic 扳机 finger in early stages when the tendon displacement causes a catching sensation. Similarly, 半脱位 lateral bands may be mistaken for sagittal band pathology if dorsal pain and snapping are present but not properly localized. Without a thorough assessment, these conditions may be misdiagnosed, leading to suboptimal treatment outcomes.
To differentiate them, location and direction of tendon displacement during resisted movement are key. Trigger finger will always involve the flexor tendon system and is palpable volarly, while sagittal band injuries produce dorsal instability at the MCP, and lateral band subluxation affects the PIP joint mechanics. Provocative testing, such as resisting MCP extension (for sagittal band), active PIP flexion (for lateral band), or palpation at the A1 pulley during finger motion (for trigger finger) can help isolate the pathology.
Accurate diagnosis also requires considering the patient’s history. Sagittal band injuries often follow a punch or hyperextension trauma, while 扳机 finger is usually atraumatic and related to overuse or inflammatory conditions. Lateral band instability may be tied to systemic illness or chronic joint stress. Imaging, including dynamic ultrasound, can further assist when diagnosis remains unclear.
In summary, although 扳机 finger, 半脱位 sagittal band injury, and 半脱位 lateral band may all present with similar symptoms, understanding their anatomical basis and performing focused physical exams allow for accurate differentiation. Early recognition is critical to guide conservative or surgical intervention and ensure optimal functional recovery.
参考
Harris, A., & Rutledge, C. (2016). Hand injuries: A practical guide to diagnosis and management. Springer.
Makkouk, A. H., Oetgen, M. E., Swigart, C. R., & Dodds, S. D. (2008). Trigger finger: Etiology, evaluation, and treatment. Current Reviews in Musculoskeletal Medicine, 1(2), 92–96. https://doi.org/10.1007/s12178-008-9012-1
Rayan, G. M., & Young, B. T. (2006). Boxer’s knuckle: Diagnosis and treatment. The Journal of Hand Surgery, 31(8), 1383–1388. https://doi.org/10.1016/j.jhsa.2006.05.009
Wolf, J. M., & Delaronde, S. (2009). Dynamic ultrasound evaluation of sagittal band injuries. Journal of Hand Surgery, 34(4), 712–715. https://doi.org/10.1016/j.jhsa.2009.01.007
更多阅读内容

使用腻子工具增强手部内在力量
我们一直在寻找增强手部内在力量的方法。人们很容易忽视这些小而强大的肌肉的重要性。它们对于执行功能性抓握模式至关重要。由于体型较小,它们可能会在短时间内变得虚弱。那么,内在强化是如何发挥作用的呢?基础…
阅读更多
化疗引起的周围神经病变中的手功能:快速回顾
Osumi, M.、Sumitani, M.、Abe、Hiroaki, A.、Otake, Y.、Kumagaya, S.-I. 和 Morioka, S. (2019)。化疗引起的周围神经病变中熟练手功能损伤的运动评估。手部治疗杂志。 (32)1、41-47。 https://doi.org/10.1016/j.jht.2017.06.003 作者:Rita Steffes The Skinny:化疗有许多持久的副作用(其中之一是化疗后手部麻木),...
阅读更多
桡骨远端骨折有目的的活动和练习期间手腕和前臂运动范围的评估
桡骨远端骨折手术修复后有目的的活动和运动练习范围内手腕和前臂运动的评估:一项随机交叉研究 Collis, J.、Mayland, E.、Wright-St Clair, V.、Rashid, U. , Kayes, N., & Signal, N. 2022。在有目的的活动和一系列……期间对手腕和前臂运动的评估
阅读更多
注册即可直接将更新发送到您的收件箱!
注册我们,我们将定期向您发送有关手部治疗的所有内容的博客文章、每次上传新视频和教程时的通知,以及讲义、协议和其他有用信息。