
鉴别诊断:扳机指 vs. 半脱位矢状带损伤 vs. 半脱位侧带损伤
手部治疗师经常会遇到一些患者,他们出现手指疼痛、弹响和肌腱滑动困难等症状。最容易混淆的情况包括: 扳机 手指, 半脱位 矢状带损伤,以及 半脱位 侧带。这些病理学涉及不同的解剖结构和生物力学破坏,但它们相互重叠的临床特征可能会使准确诊断变得复杂。了解这些病理学表现的细微差异并进行有针对性的体格检查对于制定合适的治疗方案至关重要。
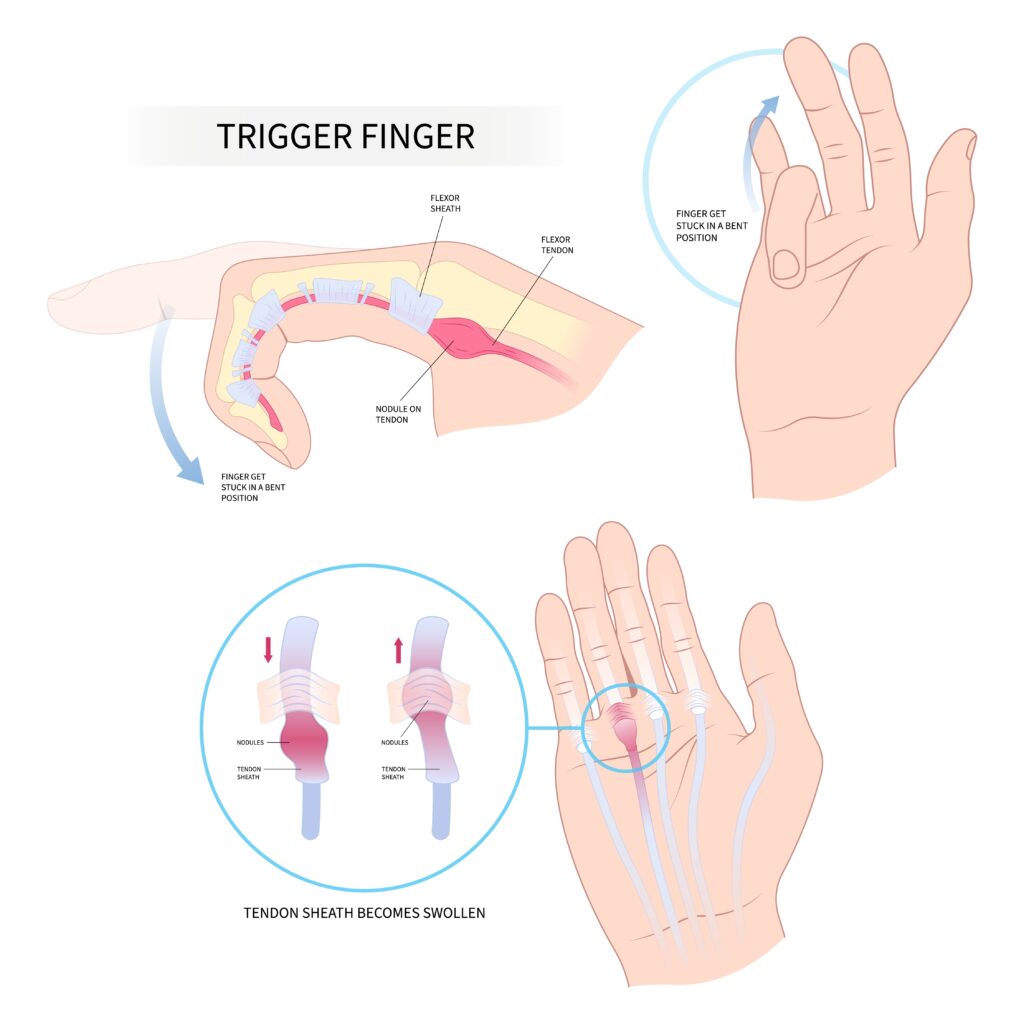
扣扳机的手指 狭窄性腱鞘炎,又称狭窄性腱鞘炎,是指屈肌腱在A1滑车处卡住的一种疾病,通常是由于肌腱或滑车系统增厚或发炎所致。患者常报告掌指关节(MCP)水平出现疼痛的卡住感或锁闭感,最常发生在中指或无名指。检查时,被动屈曲通常平稳,但主动伸展可能会遇到阻力,随后突然释放,因此“扳机”效应(Makkouk 等,2008)。触诊常可发现掌侧 MCP 皱褶处有压痛结节。
矢状带半脱位 受伤,通常被称为“拳击手指关节”,发生在矢状带无法稳定 MCP 关节上的伸肌腱时。这种情况最常见于长指,因为其活动度增加且易受创伤。临床上,患者可能会报告在 MCP 屈伸过程中出现伸肌腱弹响或移位。标志性的体格检查发现是在 MCP 受阻力屈伸时可见或可触及的伸肌腱尺侧半脱位 (Rayan & Young, 2006)。疼痛通常位于 MCP 关节的背部,并且可能出现肿胀。
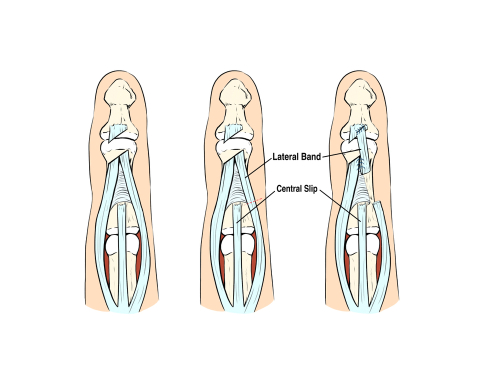
半脱位侧带 损伤较少见,常发生于患有结缔组织疾病(例如类风湿性关节炎)或创伤后的患者。导致近端指间盘(PIP)伸展的侧带,可能由于横韧带断裂或松弛而向掌侧或背侧半脱位。当向掌侧半脱位时,侧带可能充当PIP关节的屈肌而非伸肌,类似于纽扣花畸形。在检查中,治疗师可能会注意到DIP过伸时PIP屈曲,并观察主动PIP屈曲/伸展时侧带的运动。触诊可在受阻的PIP运动中检测到侧带的不稳定性 (Harris & Rutledge, 2016)。
这些情况经常被混淆,因为它们都可能出现咔哒声、MCP关节附近疼痛以及肌腱运动功能障碍。例如, 半脱位 矢状带可能模仿 扳机 早期手指肌腱移位会导致手指卡住,从而引起不适。同样, 半脱位 如果出现背部疼痛和弹响,但未明确定位,侧带病变可能会被误诊为矢状带病变。如果没有进行全面评估,这些病症可能会被误诊,导致治疗效果不佳。
为了区分它们,抵抗运动期间肌腱位移的位置和方向是关键。 扳机 手指损伤通常都会累及屈肌腱系统,且在掌侧可触及;而矢状带损伤会导致掌侧关节(MCP)背侧不稳定,而外侧带半脱位会影响近端指间关节(PIP)的力学机制。一些激发试验,例如抵抗MCP伸展(针对矢状带)、主动近端指间关节屈曲(针对外侧带)或在手指活动时触诊A1滑车(针对扳机指),有助于明确病变。
准确的诊断还需要考虑患者的病史。矢状带损伤通常是由撞击或过度伸展造成的,而 扳机 手指损伤通常无创伤性,与过度使用或炎症有关。侧带不稳定可能与全身性疾病或慢性关节压力有关。当诊断不明时,影像学检查(包括动态超声检查)可以进一步辅助诊断。
总而言之,虽然 扳机 手指, 半脱位 矢状带损伤,以及 半脱位 侧带损伤可能都表现出相似的症状,了解其解剖基础并进行有针对性的体格检查有助于准确鉴别。早期识别对于指导保守治疗或手术干预,并确保最佳功能恢复至关重要。
参考
Harris,A.,&Rutledge,C.(2016)。 手部损伤:诊断与治疗实用指南. 斯普林格。
Makkouk, AH、Oetgen, ME、Swigart, CR 和 Dodds, SD (2008)。扳机指:病因、评估和治疗。 肌肉骨骼医学的最新评论,1(2), 92–96。https://doi.org/10.1007/s12178-008-9012-1
Rayan, GM, & Young, BT (2006).拳击手指关节:诊断和治疗。 《手外科杂志》,31(8), 1383–1388。https://doi.org/10.1016/j.jhsa.2006.05.009
Wolf, JM, & Delaronde, S. (2009).矢状带损伤的动态超声评估。 《手外科杂志》,34(4), 712–715。https://doi.org/10.1016/j.jhsa.2009.01.007
3 评论
发表评论
更多阅读内容

掌腱膜挛缩症的手术和手部治疗亮点
掌腱膜挛缩症影响手部筋膜(掌腱膜挛缩症筋膜切除术手)。遇到掌腱膜挛缩症患者是比较常见的,即使这不是您治疗该患者的主要原因。患者经常在手掌中出现结节,或者甚至可能出现增粗的脐带……

手部治疗中的伤口愈合
作者:Maddie Mott 伤口愈合(治愈手疗法)涉及不同细胞类型、细胞因子介质和细胞外基质之间一系列复杂的相互作用,其四个基本阶段包括止血、炎症、增殖和重塑(Mackay & Miller,2003) 。因为成功的伤口愈合需要向伤口部位供应足够的血液和营养……

比较水肿和淋巴水肿:了解手部治疗的差异和治疗方法
比较水肿和淋巴水肿:了解手部治疗的差异和治疗方法 作为手部治疗师,我们经常遇到手臂、手和/或手指肿胀的患者,他们经常将这些症状归因于各种疾病。该领域中两个常被混淆的术语是“水肿”和“淋巴水肿”。虽然两者都涉及肿胀,但它们有不同的原因、表现形式和……

CMC 手部关节炎矫形器:力学和用途
我们在手部治疗中看到的最常见的诊断之一是第一腕掌关节的骨关节炎,掌骨与梯形的连接处。也称为基底关节关节炎(CMC 关节炎),会导致疼痛、关节畸形、力量丧失和功能丧失。患者来找我们寻求缓解症状......

注册即可直接将更新发送到您的收件箱!
注册我们,我们将定期向您发送有关手部治疗的所有内容的博客文章、每次上传新视频和教程时的通知,以及讲义、协议和其他有用信息。
感谢分享!
这篇简明扼要地分析了三种表现相似的不同情况。谢谢分享!
感谢这个简洁的总结👍🏻