
Diagnóstico diferencial: dedo en gatillo vs. lesión subluxante de la banda sagital vs. subluxante de la banda lateral
archivado en Evaluación
Diagnóstico diferencial: dedo en gatillo vs. lesión subluxante de la banda sagital vs. subluxante de la banda lateral
Los terapeutas de mano atienden con frecuencia a pacientes que presentan dolor en los dedos, chasquidos y dificultad para deslizar los tendones. Entre las afecciones que suelen confundirse se encuentran: desencadenar dedo, subluxación lesión de la banda sagital y subluxación Banda lateral. Cada una de estas patologías implica diferentes estructuras anatómicas y alteraciones biomecánicas, pero sus características clínicas superpuestas pueden dificultar un diagnóstico preciso. Comprender las sutiles diferencias en la presentación y realizar exámenes físicos específicos es crucial para una planificación adecuada del tratamiento.
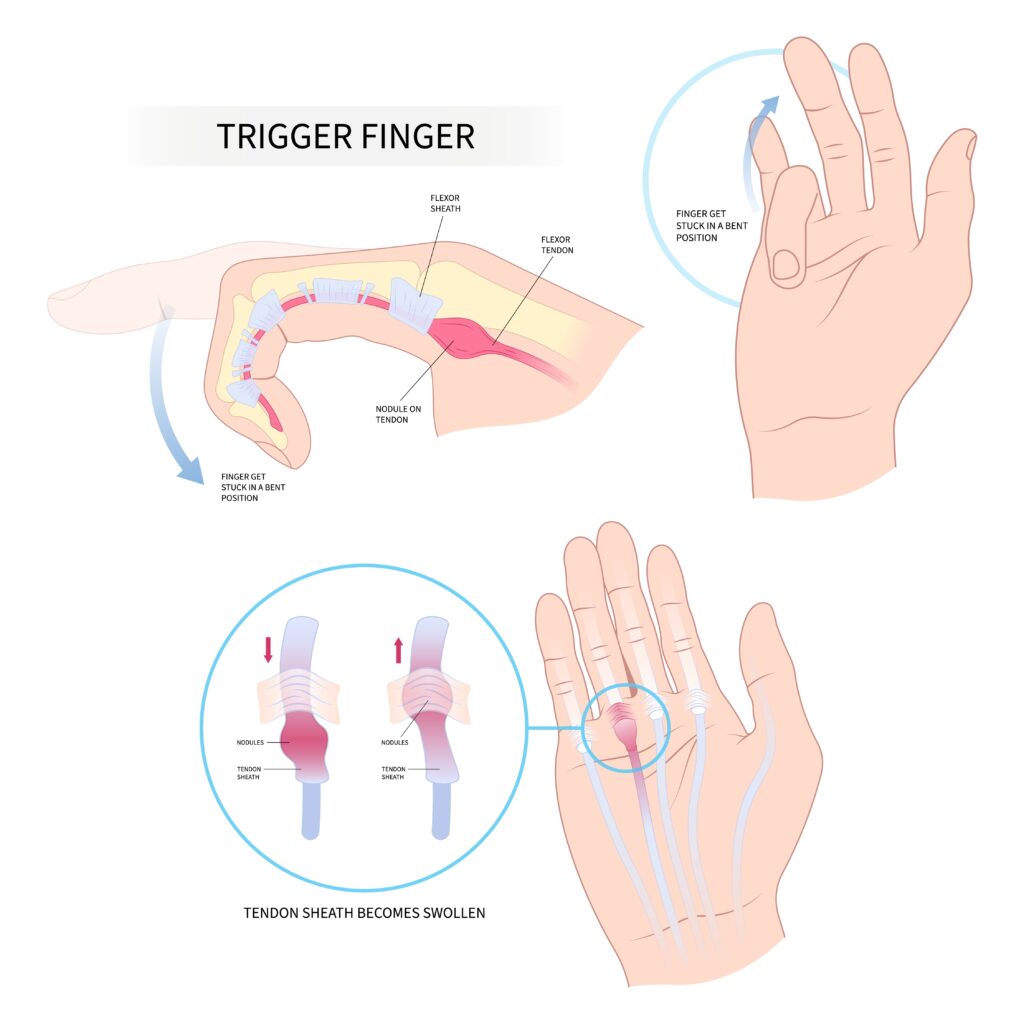
Dedo en gatillo La tenosinovitis estenosante, o tenosinovitis estenosante, es una afección en la que el tendón flexor queda atrapado en la polea A1, generalmente debido al engrosamiento o inflamación del tendón o del sistema de poleas. Los pacientes suelen referir una sensación dolorosa de atrapamiento o bloqueo a la altura de la articulación metacarpofalángica (MCF), más comúnmente en los dedos medio o anular. En la exploración, la flexión pasiva suele ser suave, pero la extensión activa puede encontrar resistencia, seguida de una liberación repentina, de ahí el término "desencadenar” efecto (Makkouk et al., 2008). La palpación a menudo revela un nódulo doloroso en el pliegue MCP volar.
Banda sagital subluxada LesiónLa luxación cubital, frecuentemente conocida como "nudillo del boxeador", se produce cuando la banda sagital no logra estabilizar el tendón extensor sobre la articulación MCF. Esta afección se observa con mayor frecuencia en el dedo medio debido a su mayor desplazamiento y susceptibilidad a traumatismos. Clínicamente, los pacientes pueden reportar chasquidos o desplazamientos del tendón extensor durante la flexión y extensión de la articulación MCF. El hallazgo característico en la exploración física es la subluxación cubital visible o palpable del tendón extensor al flexionar y extender la articulación MCF con resistencia (Rayan y Young, 2006). El dolor suele localizarse dorsalmente sobre la articulación MCF y puede presentarse inflamación.
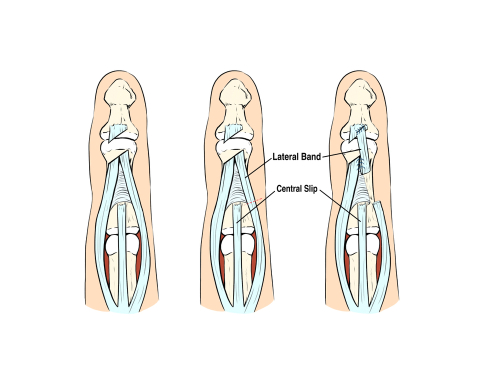
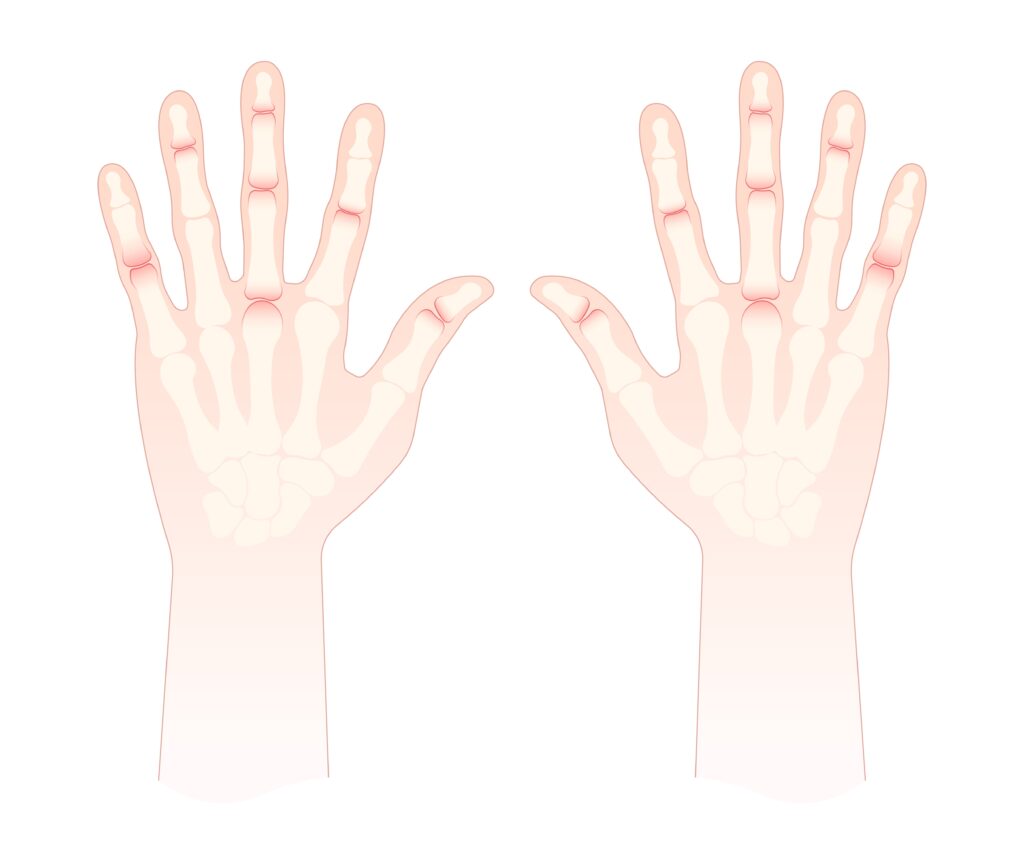
Banda lateral subluxante Las lesiones son menos frecuentes y suelen presentarse en pacientes con trastornos del tejido conectivo (p. ej., artritis reumatoide) o tras un traumatismo. Las bandas laterales, que contribuyen a la extensión de la articulación interfalángica proximal (IFP), pueden subluxarse en dirección volar o dorsal debido a la rotura o laxitud de los ligamentos retinaculares transversos. Cuando se subluxan en dirección volar, las bandas laterales pueden actuar como flexores de la articulación IFP en lugar de extensores, simulando una deformidad en ojal. En la exploración, los terapeutas pueden notar flexión de la IFP con hiperextensión de la IFD y observar el movimiento lateral de la banda durante la flexión/extensión activa de la IFP. La palpación puede detectar inestabilidad de la banda durante los movimientos de la IFP con resistencia (Harris y Rutledge, 2016).
Estas afecciones a menudo se confunden porque todas pueden presentarse con chasquidos, dolor cerca de la articulación MCF y disfunción durante la excursión del tendón. Por ejemplo, una subluxación La banda sagital puede imitar desencadenar Dedo en etapas tempranas cuando el desplazamiento del tendón causa una sensación de atrapamiento. De igual manera, subluxación Las bandas laterales pueden confundirse con una patología de banda sagital si se presentan dolor dorsal y chasquidos, pero no están bien localizados. Sin una evaluación exhaustiva, estas afecciones pueden diagnosticarse erróneamente, lo que resulta en resultados terapéuticos deficientes.
Para diferenciarlos, la ubicación y la dirección del desplazamiento del tendón durante el movimiento resistido son claves. Desencadenar El dedo siempre afecta el sistema de tendones flexores y es palpable volarmente, mientras que las lesiones de la banda sagital producen inestabilidad dorsal en la articulación metacarpofalángica (MCF), y la subluxación de la banda lateral afecta la mecánica de la articulación interfalángica proximal (IFP). Las pruebas de provocación, como la extensión resistida de la MCF (para la banda sagital), la flexión activa de la IFP (para la banda lateral) o la palpación en la polea A1 durante el movimiento del dedo (para el dedo en gatillo), pueden ayudar a aislar la patología.
Un diagnóstico preciso también requiere considerar la historia clínica del paciente. Las lesiones en la banda sagital suelen aparecer tras un traumatismo por punzón o hiperextensión, mientras que desencadenar El dedo suele ser atraumático y estar relacionado con sobreuso o afecciones inflamatorias. La inestabilidad de la banda lateral puede estar asociada a una enfermedad sistémica o estrés articular crónico. Las técnicas de imagen, incluida la ecografía dinámica, pueden ser de mayor ayuda cuando el diagnóstico no está claro.
En resumen, aunque desencadenar dedo, subluxación lesión de la banda sagital y subluxación Todas las bandas laterales pueden presentar síntomas similares. Comprender su base anatómica y realizar exámenes físicos específicos permite una diferenciación precisa. El reconocimiento temprano es crucial para orientar la intervención conservadora o quirúrgica y asegurar una recuperación funcional óptima.
Referencias
Harris, A., y Rutledge, C. (2016). Lesiones en las manos: una guía práctica para el diagnóstico y el tratamiento. Saltador.
Makkouk, AH, Oetgen, ME, Swigart, CR y Dodds, SD (2008). Dedo en gatillo: etiología, evaluación y tratamiento. Reseñas actuales en medicina musculoesquelética, 1(2), 92–96. https://doi.org/10.1007/s12178-008-9012-1
Rayan, GM, y Young, BT (2006). Nudillo del boxeador: diagnóstico y tratamiento. Revista de Cirugía de la Mano, 31(8), 1383–1388. https://doi.org/10.1016/j.jhsa.2006.05.009
Wolf, JM, y Delaronde, S. (2009). Evaluación ecográfica dinámica de lesiones de la banda sagital. Revista de Cirugía de la Mano, 34(4), 712–715. https://doi.org/10.1016/j.jhsa.2009.01.007
Comentarios sobre 3
Deja un comentario
Más para leer

¿Cuál es la eficacia de IASTM?
Citación Kim, J., Sung, DJ, Lee, J. (2017). Efectividad terapéutica de la movilización de tejidos blandos asistida por instrumentos para lesiones de tejidos blandos: mecanismos y aplicación práctica. Revista de rehabilitación del ejercicio, 13 (1). doi: https://doi.org/10.12965/jer.1732824.412 El IASTM delgado es una técnica relativamente simple que utiliza la superficie de un instrumento para minimizar la cantidad de presión o fuerza necesaria...

La importancia de las actividades con propósito después de la reparación quirúrgica de una fractura del radio distal
Por: Kelsey Melton Collis, JM, Mayland, EC, Wright-St Clair, V., Rashid, U., Kayes, N. y Signal, N. (2022). Una evaluación del movimiento de la muñeca y el antebrazo durante actividades con propósito y ejercicios de rango de movimiento después de la reparación quirúrgica de una fractura del radio distal: un estudio cruzado aleatorio. Revista de terapia de manos. https://doi.org/10.1016/j.jht.2022.07.009 The Skinny: Este estudio cruzado aleatorio...

Efectividad de la terapia conservadora y la ferulización para la primera OA de CMC
Tsehaie, J., Sprekraijse, K., Wouters, R., Slijper, H., Feitz, R., Hovious, S. y Selles, R. (2018). Resultado de una órtesis de mano y una terapia de mano para la osteoartritis carpometacarpiana en la práctica diaria: un estudio de cohorte prospectivo. Sociedad Estadounidense de Cirugía de la Mano, 1-11. La explicación: Los enfoques no quirúrgicos (terapia de mano y aparatos ortopédicos) suelen ser la opción ideal para...

Parálisis del nervio radial: una parálisis que provoca la caída de la muñeca
Parálisis del nervio radial: tratamiento

¡Regístrese para recibir actualizaciones directamente en su bandeja de entrada!
Regístrese con nosotros y le enviaremos publicaciones periódicas en el blog sobre todo lo relacionado con la terapia de manos, avisos cada vez que subamos nuevos videos y tutoriales, junto con folletos, protocolos y otra información útil.
¡Gracias por compartir!
¡Qué excelente y conciso análisis de las tres afecciones que se presentan de forma similar! ¡Gracias por compartirlo!
Gracias por este resumen conciso 👍🏻