
Cervical Spinal Cord Injuries Impact on Hand Function
Classé sous Évaluation
By: Hannah Schleining
Cervical Spinal Cord Injuries Impact on Hand Function
Le cervical region controls many of the muscles responsible for upper extremity movement,
therefore, injuries at this level can dramatically influence strength, coordination, and
independence in everyday fonction. Understanding how cervical spinal cord injuries affect upper
extremity function is essential for clinicians, caregivers, and individuals navigating recovery. By
exploring the specific challenges each level imposes we can better support meaningful
participation and improved quality of life for those living with these injuries.
C1-4: Neck, diaphragm, and sensory shoulder
Nerves: suprascapular nerves, phrenic nerve, greater and lesser occipital nerves.
Muscles: Sternocleidomastoid, deep neck muscles (postural control, head position), levator
scapulae (scapular elevation). Diaphragm impacting core stability and breathing
mechanics.
Clinical relevance: For an individual at this level of injury, they are typically total assist and will
require support during all membre supérieur tasks. Interventions for this level commonly consist of
PROM to ensure joint integrity and maintain mobility and range of motion. Therapy can focus on
adapting everyday tasks to support independent living through adaptive technology.
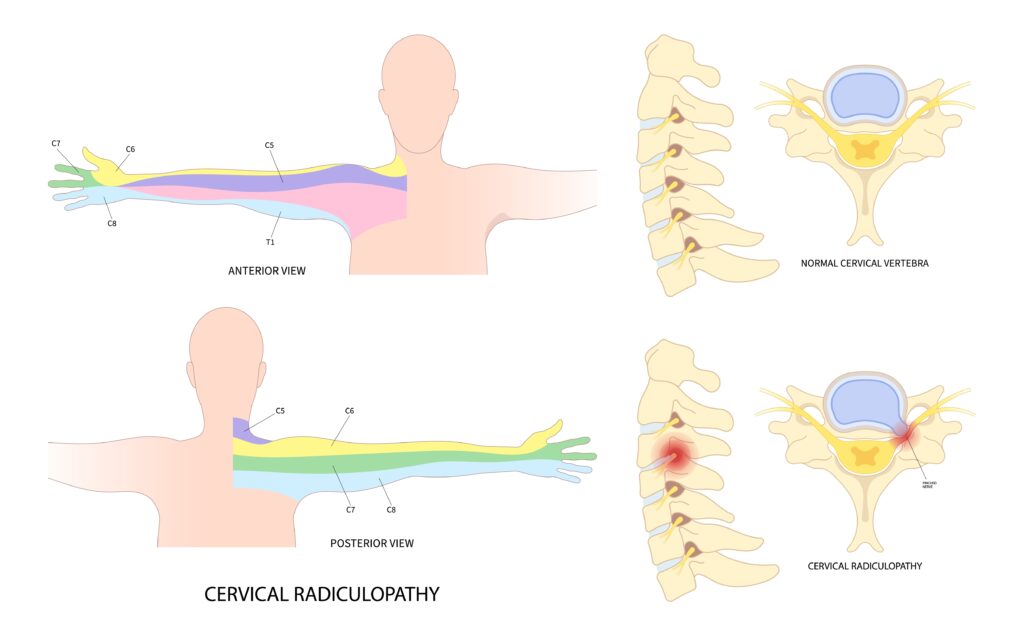
C5: Shoulder abduction, external rotation, scapular control, elbow flexion
Nerves: Axillary, suprascapular, dorsal scapular, and musculocutaneous nerves.
Muscles: Deltoid (shoulder abduction, assist with flexion and extension), supraspinatus (first 15
degrees of shoulder abduction), infraspinatus (shoulder external rotation), rhomboids (retraction
and scapular stabilization), upper fibers of levator scapulae (scapular elevation), partial biceps
brachii (elbow flexion, supination), partial brachialis (elbow flexion).
Clinical relevance: A patient will likely not be able to grasp and release objects voluntarily and
will have severely limited hand and wrist use. Adaptive equipment, such as universal cuffs or use
of an Omni-cuff should be suggested to support independence in functional tasks such as eating.
A mobile arm support can also be used to support potentially weak arm muscles. Interventions
can focus on strengthening available muscles, such as practicing elbow flexion through hand to
mouth activities for independence in self-feeding with a universal cuff.
C6: Elbow flexion, wrist extension, and thumb control
Nerves: Musculocutaneous, radial, and median nerves.
Muscles: Biceps brachii (elbow flexion and forearm supination), brachioradialis (elbow flexion),
extensor carpi radialis longus and brevis (wrist extension), supinator (forearm supination),
pronator teres (forearm pronation).
Clinical relevance: They may have difficulty using a tenodesis grasp due to lack of finger flexors and extensors, not wrist extension and therapy can focus on strengthening and improving finger flexion to improve function.
C7: Elbow extension, wrist flexion, finger extension
Nerves: Radial, median, and ulnar nerves.
Muscles: Triceps brachii (elbow extension), wrist flexors including flexor carpi radialis and
flexor carpi ulnaris, finger extensors including extensor digitorum, extensor indicis, extensor
digiti minimi, and partial wrist extensors and radial/ulnar deviators, including extensor carpi
radialis brevis and extensor carpi ulnaris. Finger flexors including flexor digitorum superficialis.
Pronator teres and pronator quadratus (forearm pronation).
Clinical relevance: Individuals may have difficulty using their arms to push for transfers,
reaching, or pushing doors open due to impact of the triceps.
C8: Finger Flexion, thumb flexion, and intrinsic hand control Nerves: Median, ulnar and radial nerves.
Muscles: Flexor digitorum profundus (DIP flexion) and flexor digitorum superficialis (PIP
flexion). Flexor pollicis longus and flexor pollicis brevis (deep head) (thumb flexion at MP and
IP). Adductor pollicis (thumb adduction). Dorsal and palmar interossei, medial two lumbricals,
hypothenar musculature (adductor digiti minimi, flexor digiti minimi, opponens digit minimi).
Lateral lumbricals and thenar muscles. Finger extensors, including extensor indicis, extensor
pollicis longus, and extensor pollicis brevis.
Clinical relevance: Due to involvement of finger flexors, gripping and making a full fist may be
difficult. Pinch and grip strength are likely limited. Additionally, impact of lumbricals and thenar
muscles can lead to decreased fine motor skills, digit control, and precise hand movements and
coordination. Functional tasks such as buttoning, using zippers and hand writing may all be
challenging.
T1: Finger abduction/Intrinsic hand
Nerves: Median and ulnar nerves.
Muscles: Dorsal interossei (finger abduction) and palmar interossei (finger adduction). Medial
and lateral lumbricals (MCP flexion and IP extension). Partial thenar muscles, including
abductor pollicis brevis, opponens pollicis, and flexor pollicis brevis (superficial head).
Hypothenar muscles, including abductor digiti minimi, flexor digiti minimi, opponens digiti
minimi. Adductor pollicis (thumb adduction).
Clinical relevance: Impact of interossei muscles can lead to “ulnar drift” or the inability to spread
fingers apart or hold a paper. Impact of lumbricals can potentially lead to clawing of fingers,
therefore, an individual may benefit from an anti-claw orthosis to improve hand function.
Involvement of thenar muscles impacts fine control of the thumb and thumb opposition. Control
of the small finger is also impacted, along with pinch strength through difficult adducting the
thumb.
The classification of injury on the ASIA Impairment Scale additionally determines a patient’s
level of function.
ASIA Impairment Scale
The classification of injury on the ASIA Impairment Scale determines a patient’s level of function and is based on the presence or absence of sacral sparing (sensory or motor function in the S4-S5 segments).
A: Complete – No sensory or motor function is preserved in the sacral segments S4-S5.
B: Sensory Incomplete – Sensory but not motor function is preserved at the most caudal sacral segments S4-S5, AND no motor function is preserved more than three levels below the motor level on either side of the body.
C: Motor Incomplete – Motor function is preserved at the most caudal sacral segments (voluntary anal contraction) OR sensory function is preserved at S4-S5, with sparing of motor function more than three levels below the motor level on either side of the body. For AIS C, less than half of key muscle functions below the single neurological level of injury (NLI) have a muscle grade ≥3/5.
D: Motor Incomplete – Motor incomplete status as defined above, with at least half (half or more) of key muscle functions below the single NLI having a muscle grade ≥3/5.
E: Normal – Sensation and motor function are graded as normal in all segments. Someone without a spinal cord injury does not receive an AIS grade.
It is important to recognize that most muscles receive innervation from multiple spinal levels, typically two or more adjacent segments, and most spinal nerve roots innervate more than one muscle. The assignment of a single muscle to one specific spinal level in clinical practice is a simplification used for standardized neurological examination purposes. Individual variation exists in the exact distribution of nerve root contributions to specific muscles, meaning that two patients with injuries at the same anatomical level may demonstrate different patterns of muscle involvement. This variability underscores the importance of comprehensive individual assessment and personalized treatment planning rather than relying solely on level-based predictions of function.
Les références:
Dahlgren, A., Karlsson, A.-K., Lundgren-Nilsson, Å., Fridén, J., & Claesson, L. (2007). Activity
performance and upper extremity function in cervical spinal cord injury patients
according to the Klein–Bell ADL Scale. Spinal Cord, 45(7), 475–484.
https://doi.org/10.1038/sj.sc.3101993
Thorsen, R., Binda, L., Chiaramonte, S., Dalla Costa, D., Redaelli, T., Occhi, E., Beghi, E., &
Ferrarin, M. (2014). Correlation among lesion level, muscle strength and hand function in
cervical spinal cord injury. European journal of physical and rehabilitation medicine,
50(1), 31–38.
Madonna Rehabilitation Hospital. (n.d.) ASIA impairment scale (AIS). Madonna Rehabilitation
Hospital. Retrieved from
https://www.madonna.org/programs/spine-injury/asia-impairment-scale-ais-score
Plus à lire

Quelle est l’efficacité de l’IASTM ?
Citation Kim, J., Sung, DJ, Lee, J. (2017). Efficacité thérapeutique de la mobilisation des tissus mous assistée par instruments pour les lésions des tissus mous : mécanismes et application pratique. Journal de réadaptation par l'exercice, 13(1). doi : https://doi.org/10.12965/jer.1732824.412 L'IASTM maigre est une technique relativement simple qui utilise la surface d'un instrument pour minimiser la quantité de pression ou de force nécessaire…

Orthèse d'arthrite CMC dans la main : mécanique et objectif
L’un des diagnostics les plus courants rencontrés en thérapie de la main est l’arthrose de la 1ère articulation carpo-métacarpienne, où le métacarpien s’articule avec le trapèze. Également connue sous le nom d’arthrite basale des articulations (arthrite CMC), elle provoque des douleurs, des déformations articulaires, une perte de force et une perte de fonction. Les patients viennent chez nous à la recherche d’un soulagement de leurs symptômes et…

Exercice thérapeutique vs activité thérapeutique
Quelle est la différence entre l’exercice thérapeutique et l’activité thérapeutique ? L'exercice thérapeutique est facturé comme 97110 et l'activité thérapeutique est facturée comme 97530. Les deux sont des codes CPT couramment utilisés dans la facturation de l'ergothérapie et de la physiothérapie. Ces codes sont très similaires et sont souvent confondus. Alors, quand et que documentez-vous pour chacun…

Comment faire une évaluation rapide mais approfondie de la thérapie de la main
Nous n'avons pas beaucoup de temps. Parfois, de nouveaux patients arrivent de manière inattendue ou quelqu'un arrive au mauvais moment et votre bloc d'une heure pour une évaluation ne dure plus que 30 minutes. Savez-vous comment tirer le meilleur parti de votre temps d'évaluation avec le patient ? Savez-vous quelles sont les choses…

Inscrivez-vous pour recevoir des mises à jour directement dans votre boîte de réception !
Inscrivez-vous avec nous et nous vous enverrons régulièrement des articles de blog sur tout ce qui concerne la thérapie des mains, des notifications chaque fois que nous mettons en ligne de nouvelles vidéos et tutoriels, ainsi que des documents, des protocoles et d'autres informations utiles.