
Biceps Tenodesis Versus Tenotomy During Arthroscopic Rotator Cuff Repair
Filed under Reviews
Article Review By: Delaney Wright
Title: Outcomes of Biceps Tenodesis Versus Tenotomy During Arthroscopic Rotator Cuff Repair: An Analysis of Patients From a Large Multicenter Database
Reference: Srinivasan, R. C., Hao, K. A., Wright, T. W., Farmer, K. W., Wright, J. O., Roach, R. P., Moser, M. W., Freidl, M. C., Pazik, M., & King, J. J. (2022). Outcomes of Biceps Tenotomy Versus Tenodesis During Arthroscopic Rotator Cuff Repair: An Analysis of Patients From a Large Multicenter Database. Orthopaedic journal of sports medicine, 10(7), 23259671221110851. https://doi-org.libproxy.nau.edu/10.1177/23259671221110851
By: Delaney Wright
The Skinny: This is a Level 3 evidence cohort study that explored the differences in pain and functional outcomes following biceps tenodesis versus tenotomy in conjunction with rotator cuff repair (RCR). A total of 1936 RCRs were included in the study with 1537 patients undergoing biceps tenodesis and 399 patients undergoing biceps tenotomy between 2013 and 2021. Outcome measures were recorded preoperatively and at 3-months, 6-months, 1-year, and 2-years postoperatively and included the American Shoulder and Elbow Surgeons Shoulder (ASES), Single Assessment Numeric Evaluation (SANE), visual analog scale (VAS) for pain, and Veterans RAND 12-Item Health Survey (VR-12). Results were categorized based on age: <55, 55-65, and >65 years and sex. Findings showed that more patients who received a biceps tenodesis with rotator cuff repair had better outcomes across all outcome measures at 2-year follow up, however, the difference did not reach the minimal clinically important difference (MCID). Overall, both procedures provide good outcomes and the decision for which procedure to undergo should be up to both the patient and surgeon.

In the Weeds: The Surgical Outcomes System (Arthrex) global database was searched for patients who had undergone a RCR in addition to either an arthroscopic biceps tenotomy or tenodesis between 2013 and 2021.
Inclusion criteria for this study was as follows:
- 2-years of follow-up
- Minimum of 1 study outcomes collected at 2-year follow-up
Exclusion criteria for this study was:
- Anyone younger than 35 years old
- Individuals undergoing open RCR, revision RCR, or rotator cuff debridement with no repair.
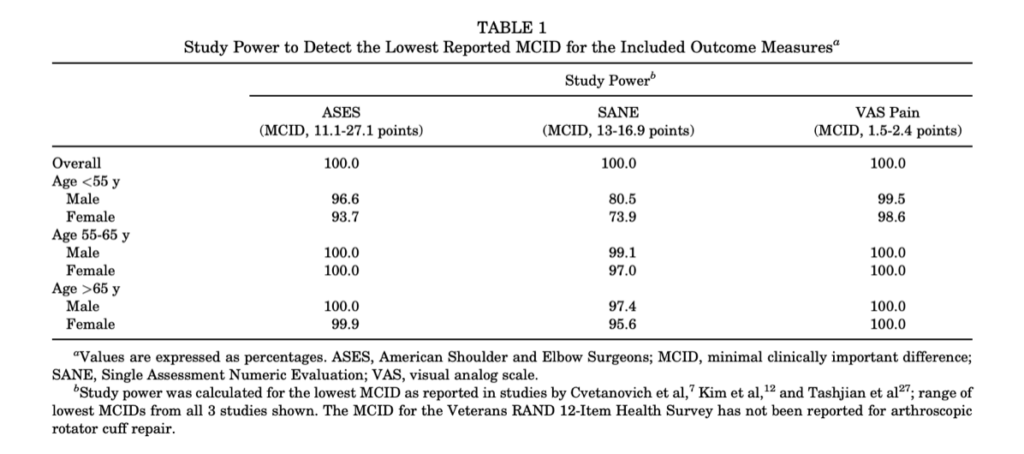
A total of 1939 patients met the inclusion criteria with primary RCR; 399 of those being in the tenotomy group and 1537 being in the tenodesis group. Patients were placed in groups based on their age with 3 groups: 35-54 years (<55 years), 55-65 years, and >65 years. Outcome measures included the ASES, a 10-point VAS for pain, the SANE, and the VR-12 Mental Component Summary (MCS) and Physical Component Summary (PCS). All outcomes were collected preoperatively and at 3-months, 6-months, 1-year, and 2-years postoperatively with the VR-12 not recorded at 3-months. The results were recorded using the chi-square test and evaluated the differences between the two groups, age group, and sex at each recording point. Additionally, preoperative and postoperative change scores were evaluated. A significance level of P < 0.05 was set and the MCID was set based on studies focused on patients undergoing arthroscopic RCR with the lowest MCID reported used to evaluate clinical significance (see Table 1). The power analysis was set based on the smallest number of patients in one group based on age and sex.
Bringing It Home:
Overall, the study found that the outcomes at the 3-month, 6-month, and 1-year postoperative follow ups were similar between the tenotomy and tenodesis group. However, at the 2-year postoperative follow-up, the tenodesis group had significantly better scores on all outcome measures compared to the tenotomy group for each patient subgroup. Of note, these differences did not meet the MCID set for the outcome measures and were not determined to be clinically significant. Additionally, the study found that females were more likely to undergo a tenotomy than males and older men were more likely to have a tenotomy than younger men. Finally, one observation of the study is that there may be a bias present towards performing tenodesis versus tenotomy with 21% of the cases being tenotomy and 79% being tenodesis. Of note, both tenotomy and tenodesis performed in conjunction with a RCR result in improved pain and functional outcomes.
Rating: This study receives a 4/5 rating. While it was a thorough review with many patients’ cases reviews, there were several possible limitations. Limitations included a lack of control over confounding variables, possible biases (selection bias, recall bias, misclassification bias), subjects were not grouped according to their biceps pathology, and additional pathology and patient characteristics were not provided. This study provides insight into our clinical practice in regard to recommending a course of surgical action when you suspect biceps pathology in combination with a RCR.
1 Comment
Leave a Comment
More To Read

Scar Wars: Scar Management Techniques
We will briefly discuss Scar Management Options and Techniques

Covid-19: What is your clinic doing?
It’s what every patient is talking about when they come in? With the suspension of every major sport, international travel banned, and hospital quarantines, everyone wants to know what their own therapists are doing to address the problem. I’m a small business owner and therapist. That means I really have 3 priorities. 1: Protect my…

Increasing Shoulder Range of Motion by improving Scapulohumeral Rhythm
Scapulohumeral rhythm is often the key component when treating shoulder conditions and the reason for the lack of total shoulder range of motion. This may also be a critical component in order to prevent shoulder conditions during rehabilitation of other upper extremity conditions such as distal radius fractures, tendon injuries, and elbow injuries. Scapulohumeral rhythm…

3 Common Reasons for Ulnar-Sided Wrist Pain and Non-Surgical Hand Therapy Treatment Options
3 Common Reasons for Ulnar Sided Wrist Pain

Sign-up to Get Updates Straight to Your Inbox!
Sign up with us and we will send you regular blog posts on everything hand therapy, notices every time we upload new videos and tutorials, along with handout, protocols, and other useful information.
Valuable article knowledge Thank you