
Therapeutic Interventions and Contraindications of Cupping
Filed under Treatments
By Kaylen Kallander
Cupping therapy is used to apply negative pressure to a localized area of muscular or neurological pain to relieve nerve pressure and increase blood flow to an affected area. This modality is commonly used for athletes, but is also a frequent treatment in physical therapy, occupational therapy, or hand therapy. While cupping can be an effective and beneficial treatment, it should be used in correct circumstances with specific precautions.
Reasons for Use
- Musculoskeletal injuries/tightness
- Myofascial adhesions
- Neurologic pain with doctor’s approval
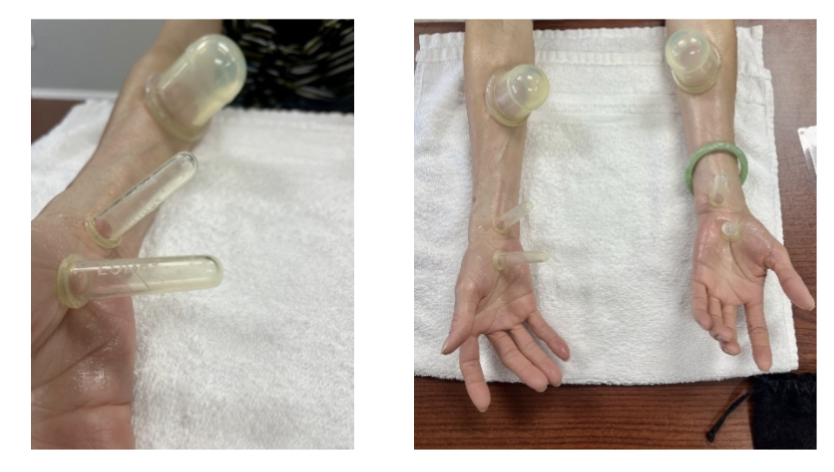
Cupping along median nerve pathways modified to use smaller cups for this patient whose arms had less surface area for suction.
Contraindications & Reasons to Discontinue
- Open wounds or acute injury with 24-72 hours
- Neurovascular compromise
- Cardiac or blood malfunction
- Blisters, lightheadedness, or significant pain during use
Considerations
In addition to the appropriate application of cupping therapy, a thorough explanation of treatment effects must be provided to patients. Patients, or parents of minor patients, should give consent before treatment proceeds. Allergies to cupping material, lotion, or oil should be considered as well. Significant bruises are expected and can last from a few days to two weeks. However, treatment should always be within a patient’s pain tolerance. While soreness is normal, it shouldn’t feel worse than having received a deep tissue massage. Patients who have received multiple treatments often present less discomfort with increased suction and decreased bruising over time. Therapeutic effects of cupping treatment can be seen with as little as 5 minutes but should be no longer than 30 minutes if in a static position.
Key Takeaways
Therapy should always be holistic, purposeful, and patient specific. Cupping may be utilized for various diagnoses and pain relief, but patient experience and preference is equally important. Furthermore, a sufficient background of medical knowledge is required to understand potential contraindications to refrain from, delay, or cease treatment. With professional critical reasoning, cupping can be a great modality to use in hand therapy for decreased muscular or nerve pain.
Cage, A. (2019). Clinical Experts Statement: The definition, Prescription, and application of cupping Therapy. Clinical Practice in Athletic Training, 2(2), 4–11. https://doi.org/10.31622/2019/0002.2
4 Comments
Leave a Comment
More To Read

Hand Therapy: How to Treat the Client with a New Distal Radius Fracture
A short blog post on the basics of treating a Distal Radius Fracture.

Changes in ROM of the MCP after Trapeziometacarpal Arthrodesis
Rapid Review: Changes in ROM of the MCP after Trapeziometacarpal Arthrodesis Hayashi, M., Kato, H., Komatsu, M., Yamazaki, H., Uchiyama, S., & Takahashi, J. (2021). Changes in the Functional Range of Motion of the Thumb Metacarpophalangeal Joint After Trapeziometacarpal Arthrodesis for Patients With Advanced Trapeziometacarpal Osteoarthritis. The Journal of hand surgery, S0363-5023(21)00613-4. Advance online publication. https://doi.org/10.1016/j.jhsa.2021.09.018. The Skinny: Several published…

A Hand Therapist’s Role in Nutrition Education for Wound Healing
By Brittany Day Role of nutrition in wound healing Nutrition plays an important function in the biological factors that contribute to normal wound healing (wound care nutrition). Patients without nutrient dense diets may experience diminished cell production, collagen synthesis, and wound contraction. There is sparse scientific evidence that explores the exact science behind nutrition and…

Management of the Stiff Finger: Evidence and Outcomes
Title: Management of the Stiff Finger: Evidence and Outcomes Reference: Yang, G., McGlinn, E. P., & Chung, K. C. (2014). Management of the stiff finger: Evidence and outcomes. Clinics in Plastic Surgery, 41(3), 501–512. https://doi.org/10.1016/j.cps.2014.03.011 Article Review By: Tommi Hintnaus The Skinny: This study focuses on understanding and managing finger stiffness, a condition characterized by…

Sign-up to Get Updates Straight to Your Inbox!
Sign up with us and we will send you regular blog posts on everything hand therapy, notices every time we upload new videos and tutorials, along with handout, protocols, and other useful information.
I love your blog posts. Short and full of little gems.
Thank you for your kind words! We love sharing.
I would add to always include active movement with your cupping treatments for best results.
That is a great tip as well!