
Hand Therapy: Does Dry Needling work to Treat Trigger Finger
Filed under Uncategorized
By: Taylor Volentine
Reference:
Azizian, M., Bagheri, H., Olyaei, G., Shadmeher, A., Okhovatpour, M. A., Dehghan, P., Jalaei, S., Sarafraz, H. (2019). Effects of dry needling on tendon-pulley architecture, pain and hand function in patients with trigger finger: a randomized controlled trial study. The Journal of Physical Therapy Science, 31. 295-298. doi:10.1589/jpts.31.295

Photo retrieved from https://www.vitalitychiropractor.com.au/dry-needling/
The Skinny:
The article seeks to address if dry needling for trigger finger is an effective mechanism to improve overall hand function and reduce pain in individuals. The medical terminology for trigger finger is known as stenosing tenosynovitis. Trigger finger displays a locked or bent position of the finger or when the finger “pops” during movement, hence the name trigger finger. When the flexor tendon sheath becomes too thick or inflamed it becomes difficult to glide through the pulley (Mayo Clinic, 2017).
Individuals who tend to participate in activities that require continuous gripping actions are at greater risk of trigger finger. If your client presents with trigger finger, they may acquire finger stiffness, finger locking and bent position, pain and tenderness of nodule surrounding the pulley, and popping or clicking during movement (Mayo Clinic 2017). Trigger finger may be treated by immobilizing the joint with a finger orthosis at the A1 pulley to promote healing, gentle exercises, avoidance of activities that involves grasping, steroid injections, and surgery if trigger finger becomes severe (Mayo Clinic, 2017).
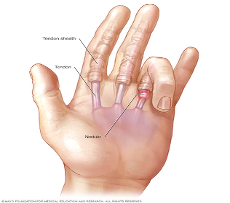
Photo retrieved from https://www.mayoclinic.org/diseases-conditions/trigger-finger/symptoms-causes/syc-20365100
In The Weeds:
This article was conducted as a randomized controlled trial with 58 participants who had trigger finger with the population ranging from 45-75 years of age. The participants were selected if they acquired the following: Unilateral idiopathic trigger finger with grade 1, 2, or 3 according to quinnell classification for at least four weeks, pain and tenderness at the location of the A1 pulley, palpation of inflamed nodule, pain and tenderness while digit flexion and extension, and locking or clicking of finger during movement (Azizian et al., 2019).
The 58 participants were randomly split evenly into two groups: the control group who did not receive dry needling treatment, and the intervention group who received dry needling treatment. The intervention group received 1 treatment of dry needling to the A1 pulley region from a therapist with 5 years of experience with dry needling and blinded to the outcomes of the study. The needle was inserted 45 degrees at the metacarpophalangeal level to nodule utilizing the fast in and fast out cone shape mechanism (Azizian et al., 2019).
Results were obtained through pre and posttest assessments measuring pain, DASH questionnaire, tendon-pulley architecture, pulley tendon thickness, and pinch grip to compare outcomes of one treatment session of dry needling. Results showed significant improvements with pain, hand function, and pulley architecture from the intervention group compared to the control group. There was not a significant difference with the control group.
Bringing It Home:
Based on the findings of this research article, trigger finger dry needling can be used as another treatment mechanism to improve overall hand function and reduce pain and pulley tendon thickness for individuals with trigger finger. Therapists may use a combination of dry needling and splinting to immobilize the movement of the A1 pulley to decrease inflammation and pain to be able to complete daily occupations.
This article portrays valuable information in regard to dry needling as an intervention to promote healing for individuals with trigger finger. This article has limitations which may have resulted in different outcomes.
· Only one dry needling treatment session providing short-term outcome data
· Limited data to compare findings
· Small sample size
Overall this article demonstrated promising data in regard to dry needling hand therapy as an effective mechanism to improve the effects of trigger finger and overall hand function. Additional research is needed to compare results with and long-term effects of dry needling.
Additional References
Mayo Clinic. (2017). Trigger Finger. Retrieved from https://www.mayoclinic.org/diseases-conditions/trigger-finger/symptoms-causes/syc-20365100
More To Read

Tennis Elbow and Graded Exercises
Lateral Elbow Pain with Graded Exercise Chronic tennis elbow with a supervised graded exercise protocol Özdinçler, A. R., Baktır, Z. S., Mutlu, E. K., & Koçyiğit, A. (2023). Chronic lateral elbow tendinopathy with a supervised graded exercise protocol. Journal of Hand Therapy, 36(4), 913–922. https://doi.org/10.1016/j.jht.2022.11.005 The Skinny: This study looked at the effectiveness of an…

Use of Proprioception in Rotator Cuff Repair
Article Review By Brittany Day Upper Limb Active Joint Repositioning During a Multijoint Task in Participants with and without Rotator Cuff Tendinopathy and Effect of a Rehabilitation Program Pairot de Fontenay, Benoit, Mercier, Catherine, Bouyer, Laurent, Savoie, Alexandre, & Roy, Jean-Sébastien. (2019). Upper limb active joint repositioning during a multijoint task in participants with and…
")
Pediatric & Adolescent Shoulder Instability
Lin, K.M, James, E.W., Spitze, E. & Fabricant, P.D. (2018). Pediatric and adolescent anterior shoulder instability: Clinical management of first-time dislocators. Current opinion in pediatrics, 30, 49-56. doi: 10.1097/MOP.0000000000000566. The Skinny: Shoulder instability for pediatric and adolescent patients is fairly common and is often complicated by a high re-dislocation rate. Shoulder instability typically occurs after…

Scapholunate Wrist Injuries in Hand Therapy
Scapholunate Wrist Injuries in Hand Therapy In outpatient hand therapy, we get a variety of referrals ranging from post-operative patients to those looking to avoid or prolong surgery. These referrals come from a variety of sources ranging from primary care doctors to experienced hand surgeons. The therapy orders can be vague to very specific. …

Sign-up to Get Updates Straight to Your Inbox!
Sign up with us and we will send you regular blog posts on everything hand therapy, notices every time we upload new videos and tutorials, along with handout, protocols, and other useful information.