
Teo, S. H., Ng D. C., Wong, Y.K.(2018). Effectiveness of proximal interphalangeal joint blocking orthosis vs metacarpophalangeal joint blocking orthosis in trigger digit: A randomized clinical trial. Journal of Hand Therapy, 1-7.
The Skinny- This study compared PIP joint immobilization via an Oval-8TM with a custom MCP blocking orthosis in the treatment of trigger finger.
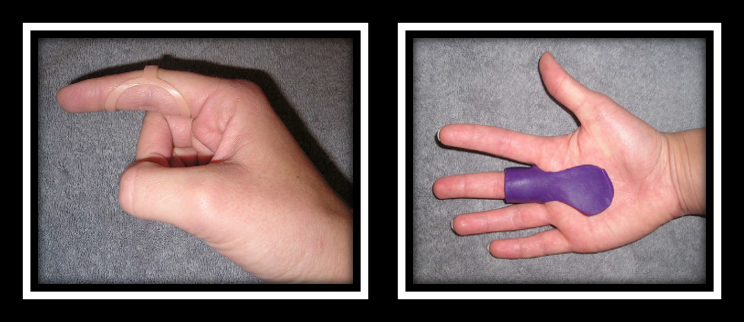
In the Weeds – Patient (n=35) with Trigger Finger (n=43) were analyzed. Twenty-three patients were allocated to the PIP joint splinting group and 20 patients were in the MCP splinting group. Patients wore the orthosis for eight weeks.
Pain reduction was observed in both groups, but pain reduction was greater with PIP joint splinting compared to the MCP joint splinting group (MCP joint splint). There was only significant improvement in QuickDASH for the PIP splinting Group. Patients wore the pip joint splint significantly longer during the day compared to the MCP splinting group (MCP splint), most likely due to improved comfort.
Bringing it Home- Findings suggest both orthoses are effective in reducing QuickDASH scores, reducing pain and improving overall trigger finger symptoms based on Green’s Classification. However, the pip joint immobilization splint was better for improved function and improved compliance.
The rationale for the rating. Small sample size. All patients with comorbidities were excluded limiting the generalizability of findings. Immobilizing the PIP joint compared to the MCP allows more function and improved compliance. When immobilizing the MCP you limit intrinsic grasp which is a necessity for function. The authors recommend wearing the orthosis for a 4-week duration of 24 hours in order to reduce triggering symptoms followed by night-time splint wear for another 3-4 weeks.
4 Comments
Leave a Comment
More To Read

Creating an Action Plan for Addressing Mental Health in the Clinic
Blog By: Rachel Reed As hand therapists, our care for our patients must be driven by the goal of treating the whole person, not just their hand or injury (Hannah, 2011). Occupational therapy is a unique profession in which we are equipped to view our patients through a holistic lens. With this lens, we are…

Dorsal Scapular Nerve Entrapment and Thoracic Pain
Don’t Forget to Evaluate for Dorsal Scapular Nerve Entrapment By Delaney Wright If your patient presents with any upper thoracic pain, it is critical to take measures to evaluate for dorsal scapular nerve entrapment. In a study completed by Sultan et al. (2013), 55 patients with interscapular pain were evaluated clinically and via nerve conduction…

Covid-19: What is your clinic doing?
It’s what every patient is talking about when they come in? With the suspension of every major sport, international travel banned, and hospital quarantines, everyone wants to know what their own therapists are doing to address the problem. I’m a small business owner and therapist. That means I really have 3 priorities. 1: Protect my…

Upper extremity weight-bearing tolerance
Barlow, S.J., Scholtz, J. & Medeiros (2020). Wrist weight-bearing tolerance in healthy adults. Journal of Hand Therapy, xxx currently in press. The Skinny Wrist pain and instability are common occurrences and can occur with acute or chronic injuries. This leads to significant dysfunction, including the inability to tolerate axial loading through the upper extremity. There is…

Sign-up to Get Updates Straight to Your Inbox!
Sign up with us and we will send you regular blog posts on everything hand therapy, notices every time we upload new videos and tutorials, along with handout, protocols, and other useful information.
Trigger finger is easy to fix with surgery release. I’ve had it done. Piece of cake.
Have seen a pt lose a finger due to a freak release surgery accident. Have seen the scar tissue left behind following a surgical release replicate a trigger digit. Have seen conservative management effectively treat a trigger digit.
Even simple surgeries carry risks for pts, especially if there are preexisting conditions like diabetes or Raynaud’s. So maybe it is best to explore all aspects of treatment before throwing out a blanket statement, right?
why go to surgery before all conservative measures? Before surgery I would certainly consider CSI, which most times resolve the situation. another thing, is inflammation in the body due yo metabolic issues also need to be considered
What are some suggestions for pediatric trigger finger in the thumb?