
Increase Shoulder Range by Improving Scapulohumeral Rhythm
Filed under Treatments
Scapulohumeral rhythm is often the key component when treating shoulder conditions and the lack of total shoulder range of motion. This may also be a critical component to prevent shoulder conditions during the rehabilitation of other upper extremity conditions such as distal radius fractures, tendon injuries, and elbow injuries.
Scapulohumeral rhythm is the rhythm in which our scapula moves in relation to the humerus in the glenohumeral joint as a means for shoulder mobility. The standard ratio is often recognized as 2:1. This means for every 2 degrees, the humerus moves; the scapula moves 1 degree. However, the ratio of scapulohumeral rhythm degrees varies among individuals.
A scapulohumeral dysrhythmia is an abnormality in a physiologic rhythm of the movement between the scapula and the humerus when moving the arm in any plane of movement. This can present in various ways, such as winging of the scapula, a shrug sign, scapular adduction, or scapular abduction during shoulder movements.
“Treatment focuses on practicing perfect reps, even if total range has to be decreased.”
Examination: The LSST
If you have a patient with a significant decrease in the shoulder range of motion in any of the movement planes, the rhythm could be a primary concern for the therapist. If the therapist suspects that this may be the problem, having the patient complete the Lateral Scapular Slide Test (LSST) can help. This can demonstrate the location of the asymmetry in the rhythm.
The 3 primary positions for the LSST are:
· Position 1, the patient’s arm is relaxed at their side (0 degrees of humeral elevation)

Position 2, the patient places their hands on the lateral iliac crest. This motion places the arm in approximately 60 degrees of abduction. Following the 2:1 ratio rule (scapulohumeral rhythm ratio), this means the humerus is responsible for 40 degrees of motion (abduction) and 20 degrees of motion on the scapula (upward rotation)

.
Position 3, shoulder abduction at 90 degrees with internal rotation. Following the 2:1 ratio rule, the humerus would be responsible for 60 degrees of motion (abduction), and the scapula would be responsible for 30 degrees of motion (upward rotation).

This quick screen can assist the therapist in identifying any scapulohumeral dysrhythmia during these aforementioned movements.
Treatment:
Treatments vary from person to person when it comes to their overall strength, range of motion, and tolerance. When a dysrhythmia is exhibited, however, some common treatments may include:
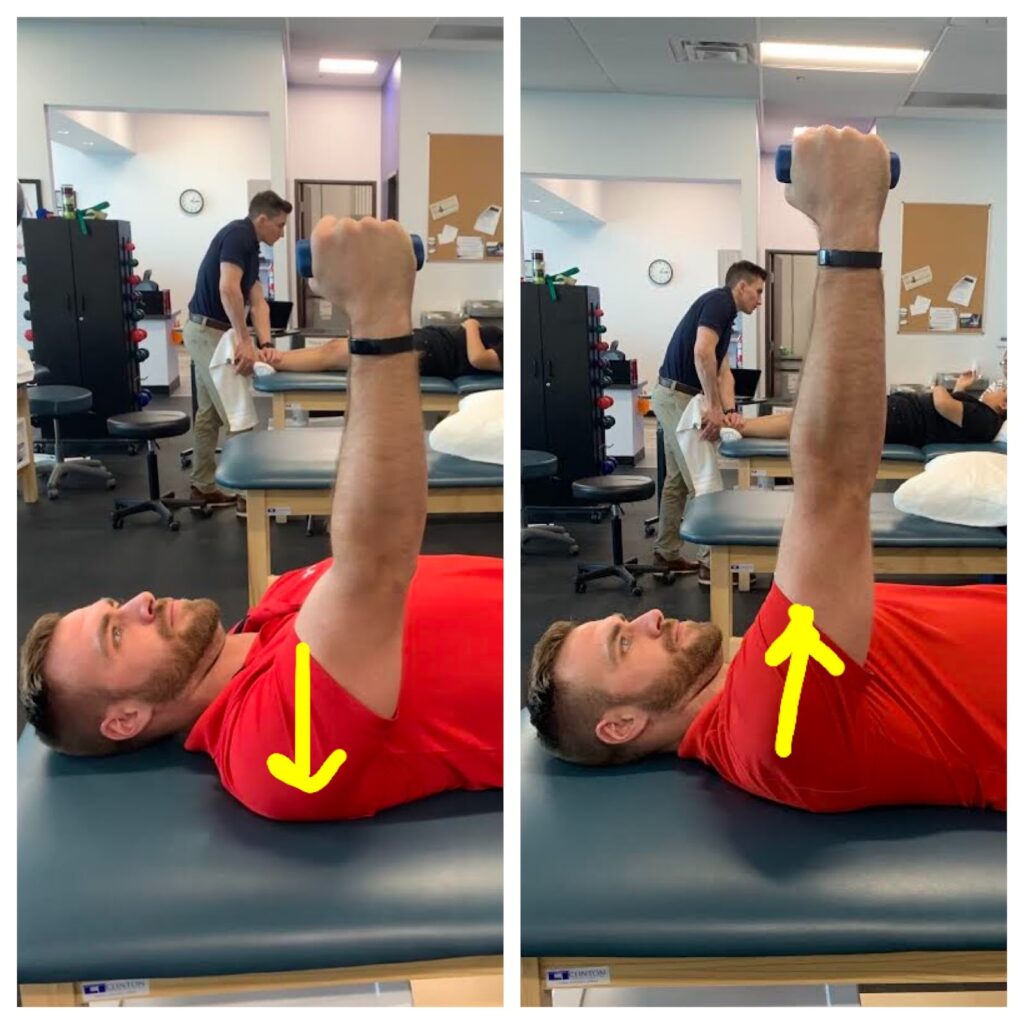
Supine punches (supine air punches) Description: With the patient supine on the therapy table, have them flex their shoulder to 90 degrees. Then have them protract the shoulder by “punching the air,” weight may also be added as patients progress
· Foam roller on the wall/table
o Description: The patient is standing facing a wall with a foam roller. They are instructed to flex their shoulder to hold the foam roller against the wall, then have them roll it up the wall while maintaining good mechanics and not allowing a shoulder hike/elevation.

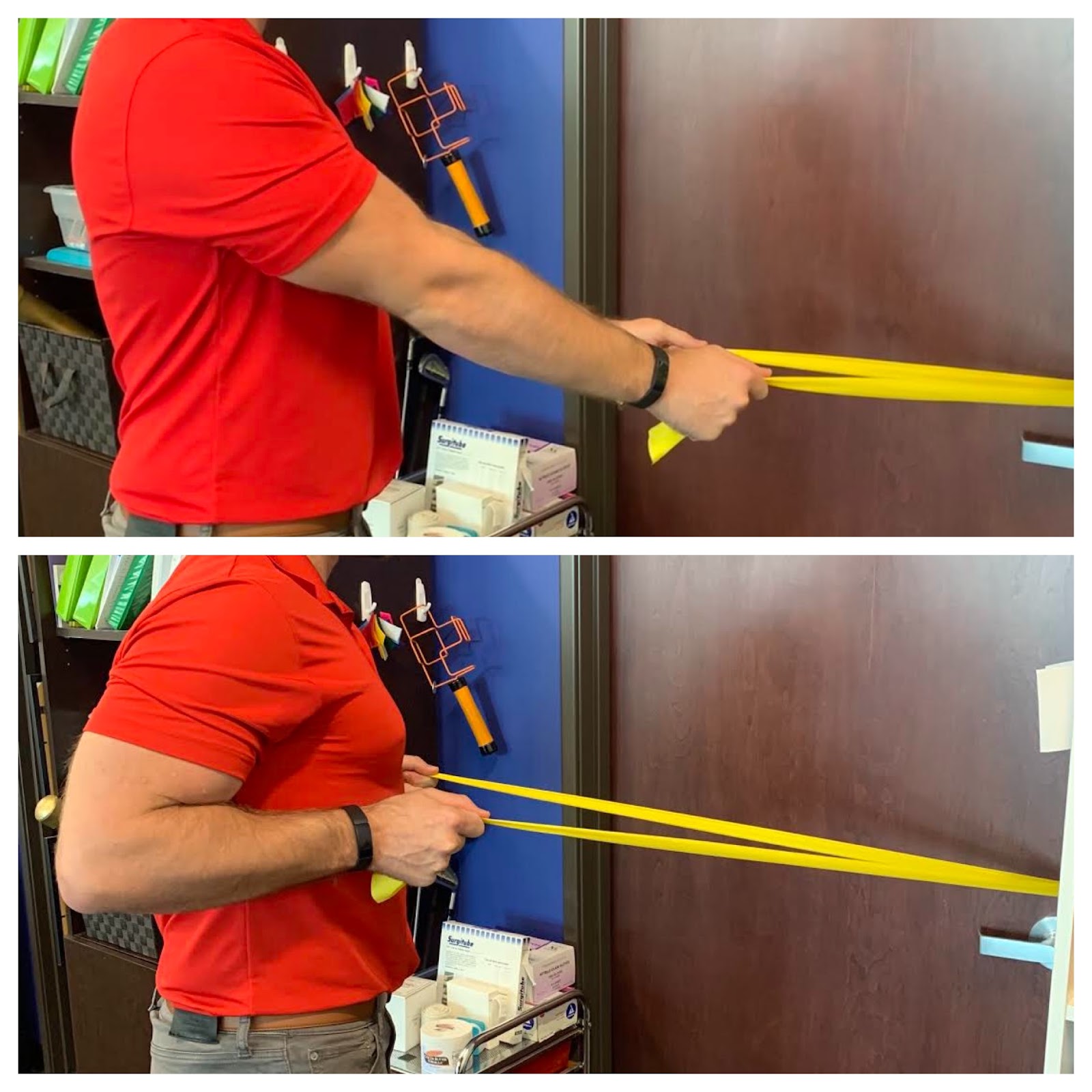
· Resisted low row pulls w/ theraband
o Description: With the patient standing facing a doorway, trap the theraband in the hinge side of the door. Have them grab the theraband ends and pull towards them (retraction) by driving the elbows back. This engages the scapular muscles while maintaining good mechanics. Do not allow a shoulder hike/elevation or a lean backward.
There are some common cues that are often given to patients which include:
“Keep your shoulder down” or
“put the shoulders in their back pockets” and/or
“hold a peanut or a dollar bill between your shoulder blades”
Mechanics are key. These treatments focus on slow controlled mechanics to improve motor planning and neuromotor recruitment to the muscles around the scapula. Treatment focuses on perfect reps, even if the total range has to be reduced. Keep an eye on the mechanics of the patient and cue as needed if mechanics degrade.
Reestablishing the typical 2:1 scapulohumeral rhythm will improve total range of motion, decrease pain and improve functional independence.
More To Read

Top 6 treatments for Pinky Fractures
Clients who have experienced a fracture of the finger or hand often find it difficult to participate in meaningful occupations. Everyday tasks from grasping items, cutting food, taking lids off containers, turning keys, and many others can be very painful. Pinky fracture is particularly challenging and painful. This is typical because the largest contributor to…

Exploring Unique Hand Anatomy
Exploring Unique Hand Anatomy The human hand is a marvel of intricate design with a combination of fine motor capabilities and strength that enable us to perform fine motor tasks ranging from delicate surgery to more gross motor tasks such as carrying heavy loads. However, no two hands are exactly alike. Anatomical variations while they…

Comparing IP and MCP joint splinting for Trigger Finger
Teo, S. H., Ng D. C., Wong, Y.K.(2018). Effectiveness of proximal interphalangeal joint blocking orthosis vs metacarpophalangeal joint blocking orthosis in trigger digit: A randomized clinical trial. Journal of Hand Therapy, 1-7. The Skinny- This study compared PIP joint immobilization via an Oval-8TM with a custom MCP blocking orthosis in the treatment of trigger finger. …
A Review on the Conservative Management of Trigger Finger
Lunsford, D., Valdes, K., & Hengy, S. (2017). Conservative management of trigger finger: A systematic review. Journal of Hand Therapy, 32(2), 212-221. https://doi.org/10.1016/j.jht.2017.10.016 The Skinny The main purpose of the literature review was to determine the efficacy of conservative management of trigger finger (TF) through the use of an orthosis in addition to therapy. The review…

Sign-up to Get Updates Straight to Your Inbox!
Sign up with us and we will send you regular blog posts on everything hand therapy, notices every time we upload new videos and tutorials, along with handout, protocols, and other useful information.