
DRUJ Instability and Hand Therapy Interventions
The distal radial ulnar joint (DRUJ) is the joint consisting of the distal radius and ulna which is held together by the ligamentous structure known as the TFC. DRUJ instability can be acute or chronic in nature. An acute injury is usually addressed by placing the patient in a long-arm cast for 6 weeks. In chronic cases, this becomes a much more complex issue and the severity depends on the reason for the chronic instability.

Conservative management of chronic DRUJ instability is often times the first line of treatment as the surgical procedures can be invasive and outcomes can vary. If an individual is very active surgical intervention is more likely to be indicated. However, a trial of therapy can be beneficial in determining if surgical intervention is needed to repair the DRUJ injury.
Functional Splinting
Conservative DRUJ injury treatment typically consists of functional bracing and is often key to successful management. You can test the stability of the joint by first applying a dorsal pressure over the ulna and a volar force on the radius. While holding the pressure over the ulna and radius, take the patient through forearm rotation. If the patient reports less pain, this is an indication they should be splinted with a dorsal pressure over the ulna and volar pressure over the radius. However, if this causes more pain, the opposite should be tested. A volar pressure should be placed over the ulna and a dorsal pressure over the radius. If there is no pain with forearm rotation, then splinting should replicate the pressure.
Therapy Interventions
When treating these patients it is very important to respect their pain as well as avoid exacerbating the symptoms. Yes, the structures can be stressed to facilitate healing however it is important to manage the stress in a slow controlled manner. Therefore having an understanding of the instability pattern and stage of injury is key to DRUJ injury treatment. It is important to keep exercises simple, once they can be performed within a pain-free range advance the patient to more challenging exercises.
Common DRUJ Injury Treatment Interventions
- Edema management techniques
- Contrast bathes for managing inflammation and pain
- Pain-free range of motion including forearm rotation, if this is painful the functional splint can be utilized while performing ROM. If still painful can begin range of motion in the dart-thrower plane.
- Isometric strengthening of PQ and ECU
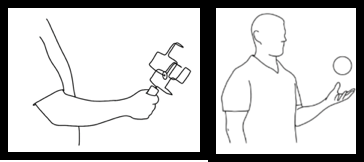
- Proprioceptive exercises advance from the joint position in space with replication to more advanced activities such as tossing a ball/disc stacker
- Once again only advance the patient if they are tolerating well and there are no exacerbation of symptoms can continue to advance with all exercises.
Treating DRUJ instability is tricky and varies based on the extent of the pathology.
Zhiqing, C. (2018) A novel staged wrist sensorimotor rehabilitation program for a patient with triangular fibrocartilage complex injury: A case report. Journal of Hand Therapy, 32, 525-533.
https://www.jhandtherapy.org/article/S0894-1130(17)30404-0/fulltext
More To Read

How to Use Translation for Improving Fine Motor Skills after a Hand Injury:
I’m always looking for new therapy ideas. I want to keep my patients interested and engaged in therapy. I also want to keep things functional and task oriented. So much of what we do with our hands is about fine motor coordination and dexterity, and that is so hard to duplicate in a clinic setting.…

IFC vs TENS: Electrical Stimulation for Pain and Swelling
In this article we’re looking at the difference between Inferential Current versus Transcutaneous Electric Nerve Stimulation (IFC vs TENS). Transcutaneous Electric Nerve Stimulation (TENS) TENS variations are often described by their technical characteristics: high frequency, low intensity (conventional TENS) or low frequency, high intensity (acupuncture-like TENS, AL-TENS) (Walsh et al., 2009). How TENS Addresses Pain:…

Video Augmented Hand Therapy after CVA with hemiplegia.
The previous rapid review discussed the positive outcomes of video-augmented hand therapy after a CVA with hemiplegia. Please watch this vlog to discover how to make the video augmented box to make it easily integrated into your clinic. Video By: Shannon Skowbo

Risk Factors for Complex Regional Pain Syndrome (CRPS) in Patients with Hand Trauma
Hand Trauma and CRPS in patients attending Hand Therapy By Tristany Hightower Savaş, S., İnal, E. E., Yavuz, D. D., Uslusoy, F., Altuntaş, S. H., & Aydın, M. A. (2018). Risk factors for complex regional pain syndrome in patients with surgically treated traumatic injuries attending hand therapy. Journal of Hand Therapy, 31(2), 250–254. https://doi.org/10.1016/j.jht.2017.03.007 The…

Sign-up to Get Updates Straight to Your Inbox!
Sign up with us and we will send you regular blog posts on everything hand therapy, notices every time we upload new videos and tutorials, along with handout, protocols, and other useful information.