
Extensor Tendon Repair Protocol (zone 4-7): Immediate Controlled Active Motion (ICAM)
Filed under Reviews, Treatments
Howell, J.W., Merritt, W. H., & Robinson, S. J. (2005). Immediate Controlled Active Motion Following Zone 4–7 Extensor Tendon Repair. Journal of hand therapy: 18, 182-90.

The Skinny- For years immobilization was the standard procedure following extensor tendon injuries in zones 4-7. As expected immobilization caused lengthy rehabilitation times, stiff joints, and tendon adhesions often leading to capsulotomy or tenolysis procedures. This study sought to provide an alternative, using an immediate controlled active motion (ICAM) protocol with a two-part orthosis program (ICAM extensor tendon protocol). A total of 140 patients took part in the study
In The Weeds- Each participant followed a three-phase rehab protocol.
Phase 1: Participants wore the two-part orthosis for 21 days, which consisted of a yoke orthosis on the involved digits with the MP joint(s) in 15-20 degrees extension, and a volar wrist orthosis with the wrist placed in 20-25 degrees of extension.
Phase 2: Participants wore the yoke orthosis at all times and wrist orthosis during medium to heavy-duty type tasks for days 22-35 post surgery.
Phase 3: Participants were to discharge the wrist orthosis entirely and only use the yoke orthosis for 36-49 post surgery. All orthoses were d/c after 49 days post surgery.
The protocol is an option when one digit is affected or two digits if not IF+LF or RF+SF. It is not recommended for 3-4 digit involvement.
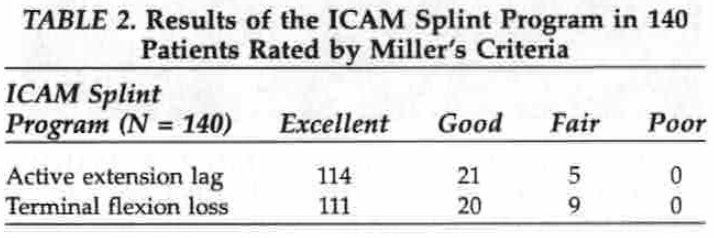
Results: No extension lag was found in 114 patients, and no terminal flexion loss was found in 111 patients. Patients that saw some extension lag or terminal flexion loss were complex tendon injuries. Grip strength at time of discharge averaged 85% of the uninjured hand. No complications such as ruptured tendons, infections, or pain syndromes occurred. No secondary surgeries such as tenolysis or capsulotomies were required.
Bringing it Home- This study demonstrated patients with extensor tendon injuries in zones 4-7 can safely perform immediate controlled active motion using a yoke splint on the fingers and a wrist extension orthosis, each with specified degrees of extension. Excellent outcomes included reducing extensor lags, return of strength, average return to work in 18 days, and an average discharge of seven weeks.
Taking into account this study’s thorough anatomical cadaver testing trials, large patient sample size, specific inclusion criteria with documentation of varying complexities of tendon injuries within its sample, and transparent data analysis, it is a reliable source to inform your practice. Detailed tutorials with pictures on how to make the two-part orthosis are also included in the text.
More To Read

The function of the Glenohumeral Joint Ligaments
Glenohumeral Joint Ligaments The Glenohumeral (GH) joint is composed of the head of the humerus and the glenoid fossa. The fossa is relatively small compared to the humeral head, making the joint highly mobile, which also leads to an increased risk of instability. The glenoid labrum is a fibrocartilagenous rim attached around the…

Scar Management in Hand Therapy
Hand therapists may feel they are in a constant battle with scar tissue. It can limit ROM, cause pain, impede other structures, and leave a less than desirable appearance. Scar tissue starts forming as early as 2 weeks after an injury and can continue forming for up to 2 years. The earlier action is taken…

Occupation Based Interventions in Hand Therapy
Keeping Occupation Based Interventions in Hand Therapy By: Tristany Hightower Are your treatments occupation based? Do you tailor your activity choices to fit the needs of each patient? As occupational therapists, we should be specialists in creating goals and interventions that are directed at returning our patients to meaningful occupations. Too often, hand therapy can…

Conservative Therapy for OA in the Fingers: A Literature Review
Beasley, J., Ward, L., Knipper-Fisher, K., Hughes, K., Lunsford, D., & Leiras, C. (2018). Conservative therapeutic interventions for osteoarthritic finger joints: A systematic review. Journal of Hand Therapy, 32. 153-164. The Skinny – The article reviews the evidence on the effectiveness of conservative treatment for those who experience osteoarthritis in fingers and in their finger…

Sign-up to Get Updates Straight to Your Inbox!
Sign up with us and we will send you regular blog posts on everything hand therapy, notices every time we upload new videos and tutorials, along with handout, protocols, and other useful information.