
Carpal fractures account for 8% of fractures in the upper extremity. The carpals are situated between the (distal radius and ulna) and the metacarpals. They make up the proximal row- Scaphoid, Lunate, Triquetrum, and Pisiform, the distal row- Trapezium, Trapezoid, Capitate, and Hamate.
Here are some of the most common carpal bone fracture
Scaphoid
The most commonly injured carpal bone in the upper extremity is the Scaphoid. It accounts for 58-66% percent of carpal fractures in adults. The scaphoid’s blood supply is a bit precarious, and if the proximal aspect of the scaphoid’s blood supply is entirely dependent on intraosseous blood flow, therefore a fracture to the proximal pole can have a lower union rate and oftentimes requires longer immobilization periods. This can also lead to avascular necrosis. If left untreated, a scaphoid nonunion advanced collapse (SNAC) may occur.
Avascular necrosis can occur at the scaphoid without any known etiology, from a wrist injury or from repetitive micro-trauma such as operating a jackhammer. Avascular necrosis of the scaphoid is known as Preiser’s Disease.
Immobilization periods for a scaphoid fracture vary on the location of the fracture as well as the patient’s unique factors. If the fracture occurs at the more distal pole, this immobilization period is typically 12 weeks. If at the proximal pole, the immobilization period is generally over 12 weeks in a long arm thumb spica.
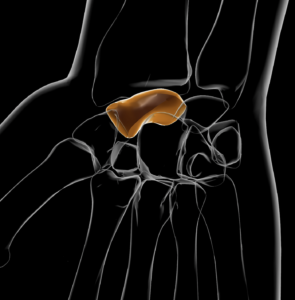
Lunate
Lunate fractures account for .5-4% of carpal fractures. They more commonly occur in individuals with a positive ulnar variance. Similar to the scaphoid, the lunate has a tenuous retrograde blood supply putting it at risk for avascular necrosis, known as Kienbock’s. This can occur after trauma, but at times the etiology is unknown. Immobilization for a lunate fracture ranges anywhere from 10-12 weeks in a long arm thumb spica. Typical, the first half of immobilization is in a cast and the second half is in a custom orthosis.
Triquetrum
Triquetrum is the second most commonly fractured carpal bone in adults and accounts for 15% of carpal fractures. Non-unions for this type of fracture are very rare and have a lower rate of complications compared to the scaphoid and lunate.
Typically these fractures are immobilized for 4-5 weeks week in a short arm cast with the thumb free.
Pisiform
Pisiform fractures are very rare and occur in less than 1% of carpal fractures. They typically occur due to a fall on the hypothenar eminence of the hand. Complications from this type of fracture include pisiform arthritis, and many will develop hypersensitivities. A padded glove can be helpful, especially if they do activities that put pressure through their palm such as riding a bike.
Immobilization periods for this type of fracture are relatively short, from 2 to 4 weeks. If a non-union occurs, the fragment can be excised.

Trapezium
The trapezium is the 3rd most common carpal fracture. This type of fracture will often occur with a distal radius fracture and 1st metacarpal fracture.
Non-displaced fractures are treated with a thumb spica cast for 4 weeks, followed by intermittent orthosis use and gentle therapy. Displaced fractures are typically treated with an ORIF.
Trapezoid
The trapezoid is a very rare carpal fracture, and the mechanics of injury usually is a result of an axially directed force along the second metacarpal. Complications typically include long-term arthritis of the STT joint.
Immobilization is typically 4-6 weeks in a thumb spica cast. If the fracture is displaced surgical fixation may be required.
There are very few publications in the literature on Trapezoid fractures due to the low etiology of occurrence.

Capitate
Capitate fractures are very rare due to the centralized location; however, in children, they are the second most common carpal fracture to occur. They typically occur in conditions with a trans-scaphoid, trans-lunate, or perilunate dislocation. Similar to the lunate and scaphoid, it has a retrograde blood supply which can lead to avascular necrosis.
Immobilization for a non-displaced capitate fracture is typically 4-6 weeks in a short arm cast.
Hamate
Hamate fractures occur in 2-4% of carpal fractures. The mechanism of injury is when a force is being transmitted through the base of the palm from an object that is gripped with force.
Treatment for a non-displaced fracture (lunate fracture treatment) is typically immobilization for 6-8 weeks in a short arm cast. If the fracture is displaced, typically, surgical intervention is required.
References
Abrego MO, De Cicco FL. Hamate Fractures. [Updated 2020 Dec 25]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2021 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK544314/
Boyce SH, Harden JL. Pisiform fracture: an uncommon wrist injury. BMJ Case Rep. 2010;2010:2132. Published 2010 Apr 20. doi:10.1136/bcr.07.2009.2132
Clementson M, Björkman A, Thomsen NOB. Acute scaphoid fractures: guidelines for diagnosis and treatment. EFORT Open Rev. 2020;5(2):96-103. Published 2020 Feb 26. doi:10.1302/2058-5241.5.190025
Guo RC, Cardenas JM, Wu CH. Triquetral Fractures Overview. Curr Rev Musculoskelet Med. 2021;14(2):101-106. doi:10.1007/s12178-021-09692-w
Guo W, Yuan B, Zhu Z, Huang C, Li R, Wu D. Non-dislocation lunate fracture combined with distal radius fracture: A case report. Medicine (Baltimore). 2018;97(49):e13574. doi:10.1097/MD.0000000000013574
Kadar A, Morsy M, Sur YJ, Akdag O, Moran SL. Capitate Fractures: A Review of 53 Patients. J Hand Surg Am. 2016 Oct;41(10):e359-e366. DOI: 10.1016/j.jhsa.2016.07.099. Epub 2016 Aug 11. PMID: 27524693.
Nammour M, Desai B, Warren M, Godshaw B, Suri M. Approach to Isolated Trapezoid Fractures. Ochsner J. 2019;19(3):271-275. doi:10.31486/toj.18.0157
Ramoutar DN, Katevu C, Titchener AG, Patel A. Trapezium fracture – a common technique to fix a rare injury: a case report. Cases J. 2009;2:8304. Published 2009 Sep 17. doi:10.4076/1757-1626-2-8304
1 Comments
Leave a Comment
More To Read

Got Wounds? How to manage them as a Hand Therapist.
Wound care is messy. It can be intimidating and scary with so many variations of wounds (for example, white skin around wounds) and so many products out there, it is hard to know what to use, when to use it, and how to use it. If you go to a wound care conference, you’ll spend most of…
Read More
Management of a TFCC Injury in Hand Therapy
By: Taylor Volentine The wrist is composed of very complex joints that assists with movement in individuals of all ages and abilities. For instance, an active individual who participates in sports such as tennis, football, or gymnastics may increase the probability for wrist complications and injury (Morrison, 2019). Individuals with repetitive trauma from work or…
Read More
3 Different Ways to Incorporate Weighted Balls into Hand Therapy Treatment Sessions:
By: Kelsey Melton 3 Different Ways to Incorporate Weighted Balls into Treatment Sessions: Weighted balls can be incorporated into hand therapy treatment sessions in various ways. This is a great therapeutic intervention for many limitations and is simple to grade up or down based on patient needs. Here are some exercise ideas to get you…
Read More
Sign-up to Get Updates Straight to Your Inbox!
Sign up with us and we will send you regular blog posts on everything hand therapy, notices every time we upload new videos and tutorials, along with handout, protocols, and other useful information.
Good brief info review of the carpal bones .