
Video-augmented mirror therapy for upper extremity rehabilitation after stroke
Filed under Treatments
Kim, H., Kim, J., Jo, S., Lee, K., Kim, J., & Song, C. (2023). Video augmented mirror therapy for upper extremity rehabilitation after stroke: a randomized controlled trial. Journal of Neurology, 270(2), 831-842.
Article Review: Shannon Skowbo
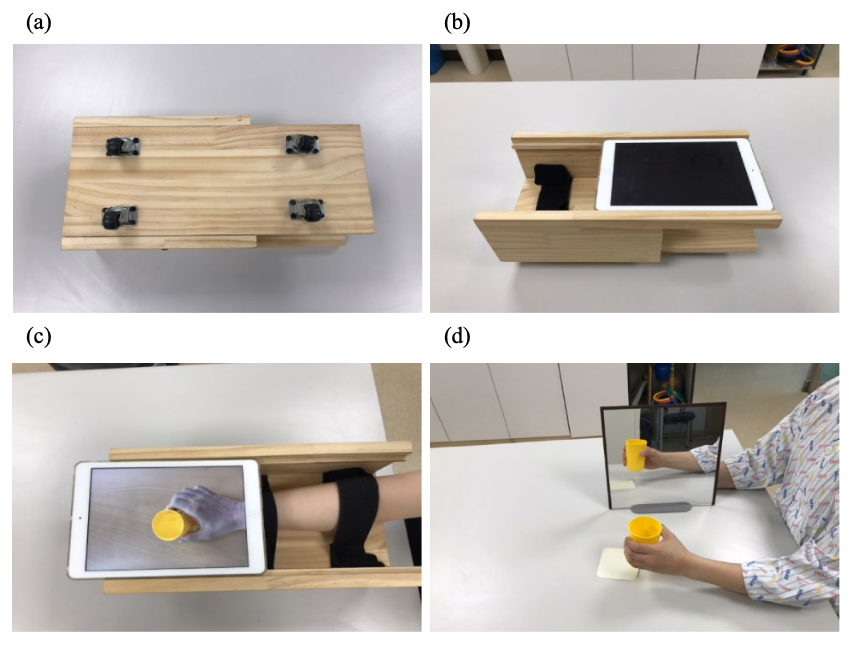
The Skinny: This single-blind, randomized control trial aimed to assess the effects of mirror therapy for stroke patients using a video-augmented device (MTVAD) on reach-to-grasp tasks and upper extremity motor function compared to traditional mirror therapy (TMT). TMT has some limitations. It requires bilateral movements since the unaffected limb produces the illusion, promotes asymmetrical postures to allow for viewing the reflection, and has discrepancies between movement performance and visual feedback. Kim et al. (2023) explores a novel therapeutic method using MTVAD to target the aforementioned limitations of TMT.
In the Weeds: Inclusion criteria included first-time stroke patients with hemiplegia during the previous 12 months, mild to moderate motor impairment as determined by upper extremity scores of 26-56 on the Fugel Myer Assessment (FMA), ability to understand and follow simple directions, and a score of greater than or equal to 21 on the Korean version of the Mini-mental State Examination. Exclusion criteria included psychiatric disorders or dementia, orthopedic disorders, apraxia or hemineglect, and prior experience with mirror therapy. Participants were randomly assigned to one of three groups: MTVAD, TMT, or the control group (conventional rehabilitation). MTVAD and TMT were performed for 30 minutes per day, 5 times per week, for 4 weeks. The control group received conventional rehabilitation for 60 minutes per day, 5 times per week, for 4 weeks. MTVAD and TMT received the same amount of conventional rehabilitation as the control group. The outcome measures included a variety of kinematic parameters during a reach-to-grasp task, upper extremity subscores on the FMA, and upper extremity subscores on the Manual Function Test (MFT). 36 participants were included in the statistical analysis.
Bringing it Home: The MVTAD group showed significantly greater improvements than the TMT and control groups in movement time, peak velocity, and trunk displacement. This means that the MVTAD group could perform the reach-to-grasp tasks more quickly, efficiently, and with a straighter trunk. The MVTAD also showed significantly greater improvements than the TMT group in FMA subscores for the shoulder, elbow, and forearm and MFT subscores for the shoulder. The improvements in kinematic parameters suggest that MTVAD “promoted better performance and upper extremity motor control ability during the reach-to-grasp movement compared to TMT in patients with stroke” (Kim et al., 2023, p. 838).
Rating: Overall, this study received a 4/5 rating. The pre-and post- test blinding, randomization, and clinically significant sample population size indicate the study has strong internal validity. However, these results can only be generalized to stroke patients who are within one year from their first stroke with only mild to moderate motor deficits.
More To Read

Distal radius fracture types seen in the hand therapy clinic
Distal radius fractures are one of the most common injuries seen in hand therapy. Several different distal radius fracture classification systems have been developed, and this blog post will focus on the more common types of distal radius fractures and their classification. Extra-articular fractures are either nondisplaced or displaced fractures. These fractures occur outside…

Does Obesity or Smoking change the outcomes for Distal Radius Fractures
Hall, Matthew J., Ostergaard, P., Dowlatshahi, A., Harper, C., Earp, B. Rozental, T. (2019). The Impact of Obesity and Smoking on Outcomes After Volar Plate Fixation of Distal Radius Fractures. The Journal of Hand Surgery. In Press, Corrected Proof, Available online 31 October 2019. Doi: https://doi.org/10.1016/j.jhsa.2019.08.017 The Skinny- Distal radius fractures are one of the…

Increase Shoulder Range by Improving Scapulohumeral Rhythm
Scapulohumeral rhythm is often the key component when treating shoulder conditions and the lack of total shoulder range of motion. This may also be a critical component to prevent shoulder conditions during the rehabilitation of other upper extremity conditions such as distal radius fractures, tendon injuries, and elbow injuries. Scapulohumeral rhythm is the rhythm in…

EDS 101: Understanding Hypermobility in the Hand Therapy Setting
EDS in the Hand Therapy Setting General Overview:Ehlers Danlos Syndrome (EDS) is a group of heritable connective tissue disorders caused bygenetic changes that affect collagen production, the protein responsible for strength and elasticityin skin, ligaments and tendons (The Ehlers Danlos Society, 2016). There are thirteen forms of EDS that each have their own set of…

Sign-up to Get Updates Straight to Your Inbox!
Sign up with us and we will send you regular blog posts on everything hand therapy, notices every time we upload new videos and tutorials, along with handout, protocols, and other useful information.