
Orthotic Intervention Incorporating Dart- Throwers Motion for Scapholunate Injury
Filed under Uncategorized
Anderson, H. & Hoy, G. (2016). Orthotic intervention incorporating the dart-thrower’s motion as part of conservative management guidelines for treatment of scapholunate injury. Journal of Hand Therapy, 29, 199-204.
By Brittany Carrie
The Skinny
Ligaments that overlay the carpal bones are imperative for wrist motion; however, are highly susceptible to instability. Injury to the scapholunate ligament is the most common cause for carpal instability resulting in altered carpal mechanics that can lead to joint degradation. Treatment can be invasive or conservative including surgery such as ligament reconstruction, direct repair, capsulodeses, or salvage repairs. Conservative treatment measures are less understood and are primarily based on the treating therapist’s clinical experience. When reviewing available research, conservative treatment protocols include use of static and controlled motion orthoses, proprioceptive exercises, and patient education for avoiding forceful gripping and weight-bearing.
Recently, there has been an increase in evidence that supports the use of dart throwers motion exercises (DTM) for scapholunate injuries. DTM is a multiplanar movement in which the wrist moves through radial extension to ulnar flexion and is seen in a variety of functional activities. These activities include drinking from a cup, hammering a nail, pouring from a carton or jug, brushing teeth, to name a few. When the wrist moves through DTM, the scaphoid and lunate bones move very little compared to uniplanar motions such as wrist extension, flexion, radial deviation, and ulnar deviation. Additionally, DTM provides proprioceptive input to mechanoreceptors in the dorsal ligaments and secondary stabilizers which in turn increases carpal stability. Thus, proprioceptive training is presumed to be a safe method of rehabilitation for a scapholunate ligament injury.
In the Weeds
A small case series was conducted to assess the outcomes of a proprioceptive rehabilitation training program that incorporated the use of a unique orthosis as a conservative treatment approach to patients who have sustained a scapholunate ligament injury. The study included 5 patients between the ages of 12 and 62 who had been diagnosed with scapholunate instability and were treated between 2008 and 2015. Patients were excluded if they opted for surgery or did not use the designed orthosis.
The orthosis included in this study was a dart-thrower’s orthosis (DTO) which was designed to limit motion within the DTM plane. Figures 1 and 2 represent the orthotic design. The DTO consisted of two parts, a distal portion that included the thumb MP joint leaving the IP joint free and a proximal portion that extended two thirds down the forearm with the distal portion
extending just proximal to the ulnar styloid. The two parts were joined together by a 0.2-mm piece of steel wire that was bent to limit movement and accurately replicate DTM to protect the scapholunate ligament from stress. The wire attached to the dorsal and palmar aspects of the forearm piece and ran through a hole that was created in the first web space. The authors achieved this position by having the patient hold a pencil and practice moving the hand as if they were throwing a dart in order to shape the wire in the correct path (dart throwing motion hand therapy).


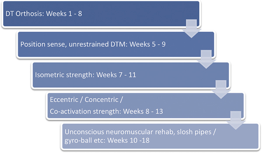
The DTO was worn at all times for 6 weeks except during therapeutic exercise and when bathing. At 4 weeks, a graded exercise program was initiated to produce active movement in the DTM plane with the DTO removed. At 6 weeks, isometric strengthening exercises were initiated for ECRB, FCR, and APL. Depending on patient tolerance, the following 6 weeks included phasing out the DTO and gradually upgrading exercises including eccentric, concentric, and coactivation strengthening, elastic resistance training, and dynamic stability strengthening exercises. Figure 3 provides a more detailed treatment outline. Limitations to the rehabilitative protocol include unspecified frequency and duration of activities and treatment variance due to symptoms of pain and instability through patient self-report and observation.
At baseline, all patients reported radial-sided wrist pain and discomfort with gripping and weightbearing. After treatment, all patients reported functional improvement and decreased pain. Clinical assessments also improved for wrist motion and gross grasp strength. Table 1 represents further details regarding pre and post-assessment results.
Table 1. Pre and post-treatment objective presentation and results.
| Patient no. | 1 | 2 | 3 | 4 | 5 |
| Pretreatment Watson’s sign | Negative | Not recorded | Positive | Negative | Not recorded |
| Post-treatment Watson’s sign | Negative | Negative | Negative | Negative | Negative |
| Pretreatment dorsal pain | Yes | Yes | Yes | Yes | Yes |
| Post-treatment dorsal pain | No | No | No | No | No |
| Pretreatment VAS | 8 | 7 | 7 (weight bearing) | 3 | 8 |
| Post-treatment VAS | 0 | 0 | 0 (weight bearing) | 0 | 0 |
| Post-treatment J2 | 22.7 (49.9 lbs) dom aff | 33 (72.6 lbs) dom aff | 41.3 (90.9 lbs) dom aff | 66.7 (146.7 lbs) dom aff | 29 (63.8 lbs) nondom aff |
| Kg (lbs) | 24 (52.8lbs) nondom | 31.3 (68.9 lbs) nondom | 36 (79.2 lbs) nondom | 56 (123.2 lbs) nondom | 26.7 (58.7 lbs) dom |
| Post DASH | 5 | 0.83 | 3.3 | 4.16 | 0 |
| Post PRWE | 0 | 1 | 11 | 0 | 0 |
VAS = visual analog pain score (0 = no pain and 10 = extreme pain); J2 = Jamar dynamometer measure of grip strength at position 2; lbs = pounds; Dom aff = dominant hand affected; Nondom aff = nondominant hand affected; Kgs = kilograms; Nondom = nondominant hand; Dom = dominant hand; DASH = Disabilities of the Arm, Shoulder, and Hand score; PRWE = Patient-Related Wrist Evaluation score.
Though this treatment protocol was successful in resolving symptoms of pain and instability and increased wrist function, the study has several limitations which cannot be overlooked. These limitations include variance in timing and details of treatment across patients with norecorded or directly monitored exercise plan, a limited number of study subjects, and no record of pre-tests in patients’ charts which prevents comparison of objective results.
Bringing it Home
Conservative treatment can be used to manage pain and instability for scapholunate ligament injuries through the use of proprioceptive training and wear of a unique orthosis design that replicates DTM.
Though there are limitations to this study, preliminary findings support further investigation of this treatment program with recommendations to compare orthotic designs and a more controlled proprioceptive-focused rehabilitation program for individuals with a scapholunate ligament injury.
1 Comments
Leave a Comment
More To Read

The Effectiveness of Manual Therapy Versus Surgery in Carpal Tunnel Syndrome
Fernández-de-las-Peñas, C., Cleland, J., Palacios-Ceña, M., Fuensalida-Novo, S., Pareja, J. A., & Alonso-Blanco, C. (2017). The effectiveness of manual therapy for carpal tunnel versus surgery on self-reported function, cervical range of motion, and pinch grip force in carpal tunnel syndrome: A randomized clinical trial. Journal of Orthopedic & Sports Physical Therapy, 47(3), 151–161. https://doi.org/10.2519/jospt.2017.7090 The…
Read More
Pros and Cons of Cortisone Injections
By: Shruti Jani Patients will often times ask the therapist their opinion on cortisone injections. Cortisone injections can be very helpful and significantly reduce inflammation, however, some therapists feel this can mask the pain not treating the true root cause of the problem. This is often debated among therapists. A short synopsis of the pros…
Read More
Test for Distal Radial Ulnar Joint of the Wrist
Ballottment Test for Wrist DRUJ Reliability and Validity Analysis of the Distal Radioulnar Joint Ballottement Test Nagashima, M., Omokawa, S., Hasegawa, H., Nakanishi, Y., Kawamura, K., & Tanaka, Y. (2024). Reliability and validity analysis of the distal radioulnar joint ballottement test. The Journal of Hand Surgery, 49(1), 15–22. https://doi.org/10.1016/j.jhsa.2023.10.006 The Skinny: Distal radioulnar joint (DRUJ)…
Read More
Sign-up to Get Updates Straight to Your Inbox!
Sign up with us and we will send you regular blog posts on everything hand therapy, notices every time we upload new videos and tutorials, along with handout, protocols, and other useful information.
Very useful, I wonder how many of these patient’s did not need surgery after completing the program.
Do you think you can provide a video of how to make the metal attachment?
Thanks