
Mechanism of Interneural Edema in Carpal and Cubital Tunnel
Filed under Diagnoses
Mechanism of Interneural Edema
Over the last few weeks I have been learning about ultrasonic imaging and carpal tunnel syndrome. When reviewing carpal tunnel syndrome, I learned that intraneural edema is a common sign of compression injuries such as carpal tunnel and cubital tunnel. There are numerous causes of carpal tunnel syndrome, and every scenario ends with the reduction of available space within the carpal tunnel and the inevitable compression on the median nerve (carpal tunnel edema). What I did not know was that chronic compression on the nerve can disrupt and open the blood nerve barrier around the perineurial layer. This allows for blood to flow freely into the nerve causing swelling or interneural edema. Since the nervous system lacks lymphatic drainage in the endoneural space, swelling inevitably increases pressure and disrupts the flow of blood to the nerve resulting in a metabolic conduction block (Cooper, 2014). One animal study found that an increase in pressure as little as 30 grams of force (about the weight of an average lightbulb) over the course of 1 hour was enough to disrupt the blood nerve barrier around the median nerve and cause diffusion (Kobayashi et al., 2005).
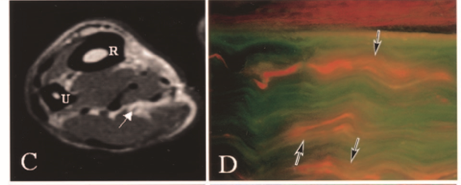
Normal Nerve No Diffusion
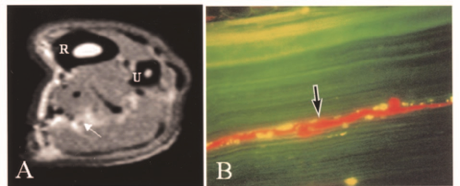
Nerve 30 Grams of Force with Diffusion
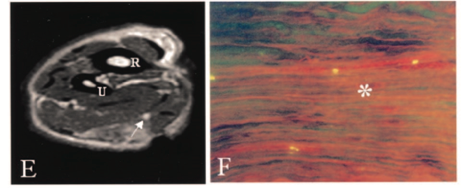
Nerve 90 Grams of Force Severe Diffusion
Chronic compression and decreased blood flow lead to impairment in nerve conduction. One source states that functional deficits are seen sequentially in the following order: motor, proprioception, touch, temperature, pain, and then sympathetic function (Cooper, 2014). Therapeutic activities such as nerve gliding exercises are hypothesized to increase nerve mobility and release the nerve from the sight of compression. Additionally, surgical decompression can help to alleviate symptoms, but the timeline for neural repair is largely based on the severity of nerve damage that has occurred. As neural edema subsides and blood flow to the nerve improves, the nerve begins to repair itself as long as the endoneurial tubes are intact. Patients are expected to regain sensation in the reverse order that they were initially lost (pain, temperature, proprioception).
Cooper, C. (20014). Fundamentals of hand therapy: Clinical reasoning and treatment guidelines for common diagnoses of the upper extremity [Second Edition]. Elsevier Mosby
Kobayashi, S., Meir, A., Baba, H., Uchida, K., and Hayakawa, K. (2005). Imaging of intraneural edema by using gadolinium-enhanced MR imaging: Experimental compression injury
2 Comments
Leave a Comment
More To Read

Neurolutions IpsiHand to Aide in Stroke Rehabilitation in Patients with Hemiparesis
Neurolutions IpsiHand to Aide in Stroke Rehabilitation in Patients with Hemiparesis Hemiparesis occurs in approximately 77% of new stroke cases and often persists into thechronic stage (Humphries et al., 2021). Recent innovation, such as brain-computer interfaces(BCIs), offer new opportunities for motor recovery even years after stroke. One such approach is the Neurolutions IpsiHand System, an…

What? I just received an order for suture removal…
How many of us have practiced suture removal in occupational or physical therapy school?? NOT I!! Often, hand surgeons will ask the therapist to remove sutures and sometimes the order will even say “remove sutures when ready” SO NOW WHAT? How to remove continuous sutures? First, we can cover the basics of sutures! There are…

Top 6 treatments for Pinky Fractures
Clients who have experienced a fracture of the finger or hand often find it difficult to participate in meaningful occupations. Everyday tasks from grasping items, cutting food, taking lids off containers, turning keys, and many others can be very painful. Pinky fracture is particularly challenging and painful. This is typical because the largest contributor to…

Creating an Action Plan for Addressing Mental Health in the Clinic
Blog By: Rachel Reed As hand therapists, our care for our patients must be driven by the goal of treating the whole person, not just their hand or injury (Hannah, 2011). Occupational therapy is a unique profession in which we are equipped to view our patients through a holistic lens. With this lens, we are…

Sign-up to Get Updates Straight to Your Inbox!
Sign up with us and we will send you regular blog posts on everything hand therapy, notices every time we upload new videos and tutorials, along with handout, protocols, and other useful information.
The inter neural edema is fascinating.
Yes is is very interesting! I agree