
By: Ammie Ingwaldson
Level 2 Fieldwork at a hand therapy clinic is a fast paced and continuous learning experience. The perfect example of this occurred last week while observing a therapist provide a client with their home CMC arthritis program. The therapist was educating the client on how to oppose their thumb to their small finger. While we watched them practice, she stated, “you have the Linburg sign!” She quickly turned to me and had me oppose my thumb to the base of my small finger, then confirmed that I had it as well. I began to become slightly concerned. We had not reviewed this sign or condition in school. I began to wonder if it was treatable and if it would affect me. My worries were put at bay when she then showed that she had it as well and provided an explanation of what it entailed.

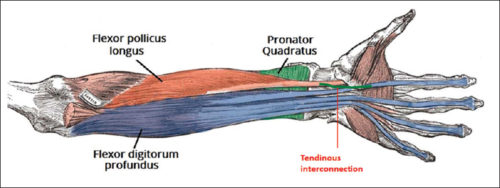
Linburg Comstock syndrome is an anatomical anomaly connecting the tendons of flexor digitorum profundus (FDP) of the index finger and flexor policis longus (FPL) (Puroshothaman & Powers, 2008). This connection of tendons leads to involuntary flexion of the index finger at the distal interphalangeal (DIP) joint with flexion of the interphalangeal (IP) joint of the thumb. The incidence of this anomaly is 37%, with higher distribution of unilateral sign than bilateral.
In most cases Linburg-Comstock syndrome is asymptomatic, but it can present as pain in the distal forearm, wrist, or hand. Median nerve symptoms, similar to carpal tunnel, can also be present due to tendon inflammation, presence of additional tendons, or synovitis with in the carpal tunnel (Puroshothaman & Powers, 2008). Individuals with repetitive thumb and finger movements, such as musicians, are more susceptible to pain or carpal tunnel like symptoms. Surgical release of the connection of FPL and FDP can be performed to relieve symptoms (Old, Rajaratnam & Allen, 2010).
References
Old, O., Rajaratnam, V., & Allen, G. (2010). Traumatic correction of Linburg-Comstock anomaly: a case report. Annals of the Royal College of Surgeons of England, 92(4), W1–W3. doi:10.1308/147870810X12659688852031
Puroshothaman, P., & Powers, D. (2008) A simple diagnostic test for symptomatic Linburg-Comstock anomaly (Linburg-Comstock test). The Internet Journal of Hand Surgery, 2(2), 1-3.
5 Comments
Leave a Comment
More To Read

Trigger Finger… Quick and Dirty!
This is for you… Hand Therapists! Stenosing tenosynovitis, otherwise known as trigger finger, is a common condition affecting children and adults of all ages. Fast Facts Trigger finger usually occurs at the A1 pulley It occurs with inflammation of the tendons and sheaths of fds and fdp The digit can lock in both flexion and…

Exertional (Chronic) Compartment Syndrome of The Hand
By: Tommi Long What is it? Chronic exertional compartment syndrome (CECS) is an exercise-induced condition affecting the muscles and nerves, leading to pain, swelling, and reduced muscle function due to increased pressure and restricted circulation. While most commonly, it impacts the arms and legs, it is rare to happen in the hand(s). CECS is most…

What is the incidence of musculoskeletal complaints in the elbow, shoulder, and neck after hand and forearm injuries?
Winiarski, L. M., Livoni, J. D., Madsen, P. V., Rathleff, M. S., & Larsen, P. (2021). Concurrent musculoskeletal complaints in elbows, shoulders, and necks after common hand and forearm injuries or conditions: A cross-sectional study among 600 patients. Journal of hand therapy: official journal of the American Society of Hand Therapists, 34(4), 543–548. https://doi.org/10.1016/j.jht.2020.05.002 The Skinny: The…

Comparison of Erb’s Palsy and Klumpke’s Palsy: Symptoms, Presentation, and Treatment Options
What is the brachial plexus? The brachial plexus is a group of nerves originating from the cervical and thoracic nerve roots (from C5 to T1). The brachial plexus forms 5 peripheral nerves of the upper extremity, consisting of the musculocutaneous, median, radial, ulnar, and axillary nerves. This group of nerves supplies motor and sensory innervation…

Sign-up to Get Updates Straight to Your Inbox!
Sign up with us and we will send you regular blog posts on everything hand therapy, notices every time we upload new videos and tutorials, along with handout, protocols, and other useful information.
I love that great fun fact with a quick explanation, great visual representation of the UE possible problems, and treatment options that are available.
Thanks.
I have this issue but not just one or two fingers is every finger in both hands. if i bend thumb even my little finger goes with it. Just wondering how rare it is for that to happen?
Thanks for sharing! Funny enough, I also found out I had this anomaly during my level 1 OT fieldwork rotation at a hand therapy clinic! Actually, I realized I had this involuntary flexion of the index finger when I was young, in girl scouts, and I was unable to do the girl scout hand sign without my pointer finger bending. I forgot about it until my fieldwork rotation, where I found out the name of what it was and why it occurs! So, I guess another clinical test option could be to have the client try to do the girl scout hand sign 😂
I have it slightly on the right side, but extremely pronounced on the left side, which I only noticed after my left wrist broke and was surgically repaired with a metal plate. I can’t flex my left thumb without the 2 farthest joints of left index flexing all the way down. Can surgery or tge original injury make this condition worse?
I would recommend seeing a doctor as we are not really allowed to give out specific medical advise on this platform. Thanks