
Pillar Pain After Carpal Tunnel Release Surgery
Carpal tunnel release (CTR) surgery is a common procedure, with the majority of patients experiencing satisfaction with its outcomes. However, for some individuals, a temporary complication known as “pillar pain” may arise, affecting approximately 13% of those undergoing CTR.

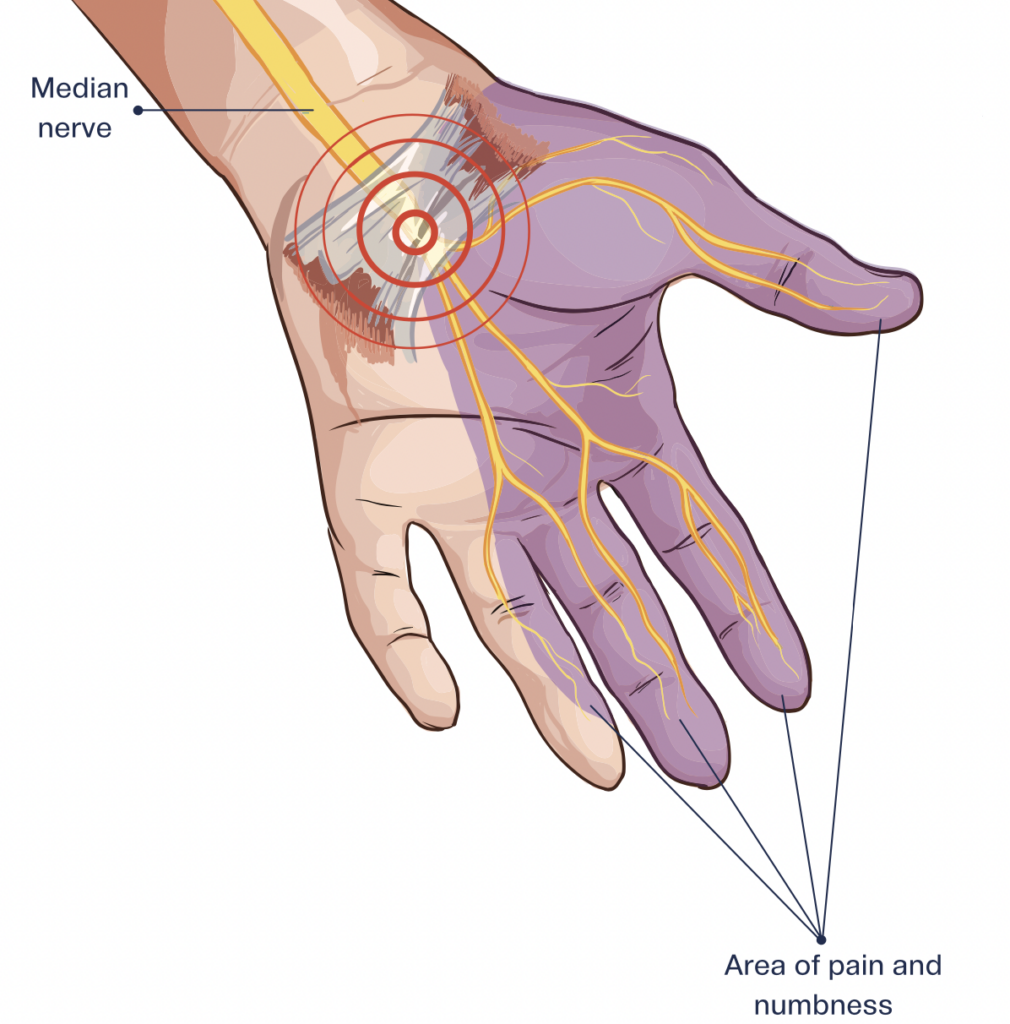
Pillar pain manifests in the thenar eminence and hypothenar eminence due to their proximity to the transverse carpal ligament. It is characterized by wrist pain that causes tenderness and discomfort upon touch, distinct from the incision pain typical of surgical recovery, which usually subsides within a few days to weeks.
Although pillar pain symptoms typically resolve within three months, they can persist longer, even up to 9-12 months. While the exact cause of pillar pain remains elusive, several theories have been proposed, including tender scar tissue, muscle alignment alterations, joint inflammation, injury to small nerve fiber branches, and nerve irritation. Notably, a neurogenic component is suggested, indicating that nerve tissue damage from carpal tunnel surgery may play a significant role.
A theory posits that avoiding the “critical pillar rectangle” during surgery, which encompasses specific anatomical landmarks, could substantially reduce the likelihood of pillar pain occurrence.
Hand therapists offer various interventions for managing pillar pain, including:
- Stretching exercises such as the extrinsic stretching of wrist/hand flexor and tendon gliding exercises.
- Soft tissue mobilization targeted at the thenar and hypothenar eminences, gradually increasing pressure in sensitive areas.
- Desensitization techniques involve the use of different textures like cotton, wool, foam, soft Velcro, and others to rub over sensitive areas. Immersion of the affected area in substances like cotton balls, foam, rice, or beans can aid in desensitization.
- Median nerve glides to facilitate nerve flossing and restore median nerve mobility.
- Scar softening treatments such as paper tape or silicone gel pad.
By employing these strategies, individuals experiencing pillar pain can effectively manage their symptoms and facilitate recovery following carpal tunnel surgery.
Kumar, A., & Lawson-Smith, M. (2024). Pillar pain after minimally invasive and standard open carpal tunnel release: A systematic review and meta-analysis. Journal of Hand Surgery Global Online. https://doi.org/10.1016/j.jhsg.2023.12.003
Ludlow, K., Merla, L., Cox, J., & Hurst, L. (1997a). Pillar pain as a postoperative complication of carpal tunnel release. Journal of Hand Therapy, 10(4), 277–282. https://doi.org/10.1016/s0894-1130(97)80042-7 .
2 Comments
Leave a Comment
More To Read

Putting Occupation in Hand Therapy
It was early in my career, maybe a year out of school. I was working with a veteran physical therapist that had been practicing for thirty plus years. She was somewhat intimidating and one of those old school physical therapists that thrived on being aggressive. We were chatting about what areas of occupational hand therapy…

Splinting vs Stretching after a Stroke to treat Hand Spasticity
Splinting versus Stretching to improve hand function and reduce hand spasticity after stroke Reference: Ahmad Khan, M., & Singh, P. (2018, February). Effect of Hand Splinting versus Stretching Exercises for Reducing Spasticity and Improving Hand Function in Poststroke Hemiplegia: AComparative Interventional Study. Retrieved December 4, 2022, fromhttps://www.ijotonweb.org/article.asp?issn=0445 -7706;year=2018;volume=50;issue=4;spage=125;epage=129;aulast=Khan The Skinny: A comparative study by Khan…

Shoulder Pain: The Effectiveness of Conservative Treatment
Reference: Steuri, R., Sattelmayer, M., Elsig, S., Kolly, C., Tal, A., Taeymans, J., & Hilfiker, R. (2017). Effectiveness of conservative interventions including exercise, manual therapy and medical management in adults with shoulder impingement: a systematic review and meta-analysis of RCTs. British journal of sports medicine, 51(18), 1340–1347. https://doi.org/10.1136/bjsports-2016-096515 By: Tayler Roost The Skinny: This study…

“Do joint mobilizations assist in the recovery of lateral elbow tendinopathy? A systematic review and meta-analysis”
By Sophia Grimm Lucado, A. M., Dale, R. B., Vincent, J., & Day, J. M. (2019). Do joint mobilizations assist in the recovery of lateral elbow tendinopathy? A systematic review and meta-analysis. Journal of hand therapy : official journal of the American Society of Hand Therapists, 32(2), 262–276.e1. https://doi.org/10.1016/j.jht.2018.01.010 The Skinny: The purpose of this study was…

Sign-up to Get Updates Straight to Your Inbox!
Sign up with us and we will send you regular blog posts on everything hand therapy, notices every time we upload new videos and tutorials, along with handout, protocols, and other useful information.
Thank you for all the info
Great information, thanks! 🙏🏻