
Written by Melissa Miller
Introduction
Volkmann’s contracture is a rare condition that occurs after injury to the elbow and upper arm, typically from a crush injury. This condition can occur when acute compartment syndrome is left untreated. If unrecognized, Volkmann’s contracture can lead to a permanent deformity in the hand and forearm. Hand therapists are one of the providers who see patients in frequent and regular intervals after the onset of injuries. This makes them critical in the role of identifying and intervening if Volkmann’s contracture begins to develop. This post will discuss what Volkmann’s contracture is, the muscles that are affected, and what it may look like throughout its stages of severity.
Volkmann’s Contracture and Cause
Volkmann’s contracture is a permanent flexion deformity at the hand and wrist that has a claw-like presentation. Volkmann’s contracture is caused by acute arterial insufficiency to the arm. [2, 3] Most commonly, this arterial insufficiency is caused by compartment syndrome that occurs after an individual has experienced trauma to the arm (between shoulder and elbow) or at the elbow. Compartment syndrome is a condition where there is an increase of intra-facial compression in a closed compartment. [2, 3] Volkmann’s contracture develops from acute compartment syndrome if the compartment is not released, thus causing decreased blood flow and oxygen (arterial insufficiency) to the forearm as well as suppresses nerves within the compartment. When blood supply and oxygen are not able to supply muscles for an extended amount of time it has severe effects on those muscles. These effects include the shortening of the muscles and loss of function. With compartment syndrome causing arterial insufficiency and compression of nerves it results in muscle and nerve necrosis. [2, 3]. This necrosis then can transition into fibrosis within the muscle and calcification in the later stages. Compression of nerves can also lead to high ulnar and median nerve palsy.
Primary Muscles Involved
- Superficial Muscles of forearm: Pronator teres, flexor carpi radialis, palmaris longus, flexor carpi ulnaris, flexor digitorum superficialis
- Deep Muscles of the forearm: Flexor pollicis longus, pronator quadratus, flexor digitorum profundus
Contracture Severity, Presentation of Hand, and Treatment
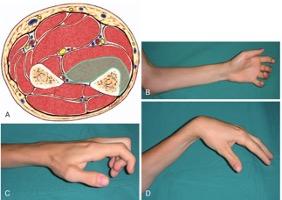
Mild Contracture:
[4]
- Muscles: localized contracture, only involving parts of flexor digitorum profundus (cross-sectional diagram picture A)
- Clinical Presentation: flexion contracture in 2-3 fingers, typically including the long finger and ring finger (picture B, C, D)
- Sensory Effects: none – min sensory loss
- Therapeutic Volkmann’s contracture treatment: PROM stretching, progressive splinting, AROM exercises
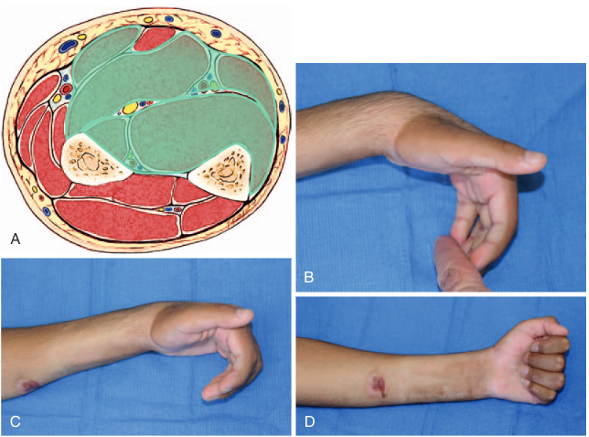
Moderate Contracture:
[4]
- Muscles: flexor digitorum profundus and flexor pollicis longus, may also include some of the superficial muscles such as flexor carpi radialis, flexor carpi ulnaris, and flexor digitorum superficialis (cross-sectional diagram picture A)
- Clinical Presentation: presents as claw hand with flexion at all digits and palmar wrist flexion (picture B, C, D)
- Sensory Effects: moderate sensory deficits in median n. and ulnar n. (more in median n.)
- No therapeutic treatment, requires surgery
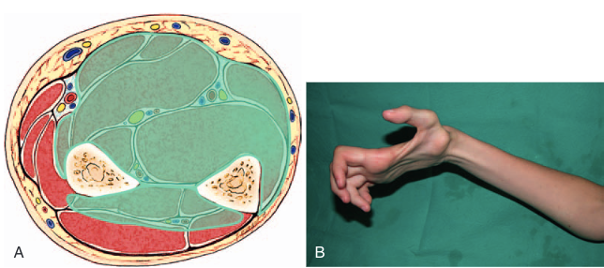
Severe Contracture:
[4]
- Muscles: contractures in most extensor muscles and all flexor muscles of the forearm (cross-sectional diagram picture A)
- Clinical Presentation: severe contracture deformities, intrinsic muscle dysfunction (picture B)
- Sensory Effects: pronounced sensor deficits from median n. and ulnar n.
- No therapeutic treatment, requires surgery
Signs of Volkmann’s Contracture:
There are 5 signs that an individual will have with Volkmann’s contracture. These signs show throughout different severities of the condition; however, the earlier signs can help you identify as a clinician that the client’s symptoms may point to Volkmann’s contracture. The 5 signs have been referred to as the 5 Ps. [3] These include:
1. Pain
2. Pallor
3. Pulselessness
4. Paresthesia
5. Paralysis
Conclusion
Pain is the first sign in Volkmann’s contracture. A patient will start to feel pain with palpation over the affected area of the forearm. If you have a patient who is starting to have flexor stiffness in 2-3 digits and they have pain when palpating the arm, this may be a sign that the patient is beginning the early stages of Volkmann’s contracture. As the condition progresses the individual may show pallor where their skin looks bleached, as well as present as pulselessness, where you are unable to feel a pulse in the distal forearm. If the patient is in the moderate and severe stages, this is when they will show the signs of paresthesia, decreased sensation, and observable muscle paralysis.
Hand therapists are one of the few professionals who see individuals on a regular basis after injury. If compartment syndrome has gone unrecognized by physicians at early follow-ups, and mild Volkmann’s contracture begins to develop, a hand therapist may be the one most likely to catch it before it progresses into stages that require surgery. It is important that the clinician knows what Volkmann’s contracture is, as well as what the signs and symptoms are so they are able to catch it in time. If caught in the early stages, PROM, progressive splinting, and AROM exercises are key. If not addressed until later stages, then referral back to the surgeon may be necessary for surgical intervention.
Resources
[1] Clinic, B. (2018, May 25). Volkmann’s ischemic contracture flexor slide surgery. Retrieved November 24, 2020, from https://brahmanandclinic.blogspot.com/2018/05/volkmanns-ischemic-contracture-flexor.html
[2] Mirza TM, Shrestha AB. (2020) Volkmann Contracture. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing. Available from: https://www.ncbi.nlm.nih.gov/books/NBK557754/
[3] Physiopedia. (n.d.). Volkmann’s contracture. Retrieved November 10, 2020, from https://www.physio-pedia.com/Volkmann’s_Contracture
[4] Stevanovic, M. V., & Sharpe, F. (2017). Compartment Syndrome and Volkmann Ischemic Contracture. In S. W. Wolfe, R. N. Hotchkiss, W. C. Pederson, S. H. Kozin, & M. S. Cohen (Authors), Green’s operative hand surgery (pp. 1763-1787). Philadelphia, PA: Elsevier.
More To Read

Video Augmented Hand Therapy after CVA with hemiplegia.
The previous rapid review discussed the positive outcomes of video-augmented hand therapy after a CVA with hemiplegia. Please watch this vlog to discover how to make the video augmented box to make it easily integrated into your clinic. Video By: Shannon Skowbo

How to Strengthen the Intrinsics with Puttycise Tools:
How to strengthen the intrinsic with Puttycise tools

The function of the Glenohumeral Joint Ligaments
Glenohumeral Joint Ligaments The Glenohumeral (GH) joint is composed of the head of the humerus and the glenoid fossa. The fossa is relatively small compared to the humeral head, making the joint highly mobile, which also leads to an increased risk of instability. The glenoid labrum is a fibrocartilagenous rim attached around the…

Splinting and Stretch Protocol for Pediatric Trigger Thumb
Tan, A. C., Lam, K. S., & Lee, E. H. (2002). The Treatment Outcome of Trigger Thumb in Children. Journal of Pediatric Orthopaedics B, 11(3), 256-259. The Skinny:Pediatric trigger thumb is a “relatively uncommon” condition of unknown origins. Studies have indicated that spontaneous recovery of trigger thumb is around 25-40%, and chances increase with age.…

Sign-up to Get Updates Straight to Your Inbox!
Sign up with us and we will send you regular blog posts on everything hand therapy, notices every time we upload new videos and tutorials, along with handout, protocols, and other useful information.