
Which is better: Splinting the MCP or PIP joint when managing Trigger Finger?
Filed under Orthoses, Treatments
Teo, S. H., Ng D. C., Wong, Y.K.(2018). Effectiveness of proximal interphalangeal joint blocking orthosis vs metacarpophalangeal joint blocking orthosis in trigger digit: A randomized clinical trial. Journal of Hand Therapy, 1-7.
The Skinny- This study compared PIP joint immobilization via an Oval-8TM with a custom MCP blocking trigger finger orthosis treatment.
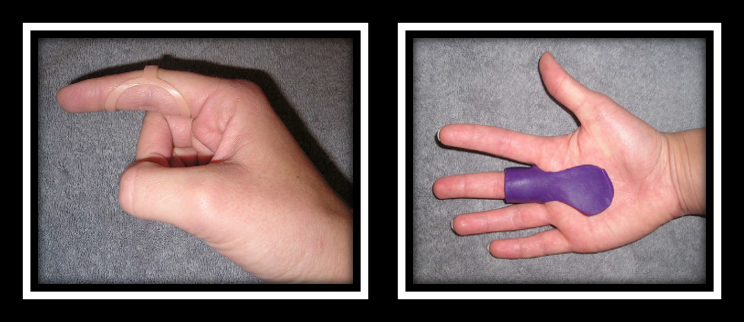
In the Weeds – Patient (n=35) with Trigger Finger (n=43) were analyzed. Twenty-three patients were allocated to the PIP joint splinting group and 20 patients were in the MCP splinting group. Patients wore the orthosis for eight weeks – these were MCP splint for trigger finger, MCP blocking splint and pip joint splint.
Pain reduction was observed in both groups, but pain reduction was greater with PIP joint splinting compared to the MCP joint splinting group. There was only significant improvement in QuickDASH for the PIP splinting Group. Patients wore the pip joint splint significantly longer during the day compared to the MCP splinting group, most likely due to improved comfort.
Bringing it Home- Findings suggests both orthoses are effective in reducing QuickDASH scores, reducing pain and improving overall trigger finger symptoms based on Green’s Classification. However, the pip joint immobilization splint was better for improved function and improved compliance.
Rationale for rating. Small sample size. All patients with comorbidities were excluded limiting the generalizability of finding. Immobilizing the PIP joint compared to the MCP allows more function and improved compliance. When immobilizing the MCP you limit intrinsic grasp which is a necessity for function. The authors recommend wearing the orthosis for a 4 week duration for 24 hours in order to reduce triggering symptoms followed by night-time splint wear for another 3-4 weeks.
10 Comments
Leave a Comment
More To Read

Article Review: Relative Motion for Extensor Tendon Repair zone V-VI? Is a night-time resting hand orthosis beneficial?
Hirth, M. J., Hunt, I., Briody, K., Milner, Z., Sleep, K., Chu, A., Donovan, E. & O’Brien, L. (2021). Comparison of two relative motion extension orthotic programs following surgical repair of finger extensor tendons in zones V-VI: A randomized equivalence trial. Journal of Hand Therapy-to be published. The Skinny: Following a zone V-VI tendon repair,…

Comparison of Erb’s Palsy and Klumpke’s Palsy: Symptoms, Presentation, and Treatment Options
What is the brachial plexus? The brachial plexus is a group of nerves originating from the cervical and thoracic nerve roots (from C5 to T1). The brachial plexus forms 5 peripheral nerves of the upper extremity, consisting of the musculocutaneous, median, radial, ulnar, and axillary nerves. This group of nerves supplies motor and sensory innervation…

THE SENSITIVITY AND SPECIFICITY OF ULTRASOUND FOR THE DIAGNOSIS OF CARPAL TUNNEL SYNDROME: A META-ANALYSIS
Fowler, J. R., Gaughan J. P., & Ilyas, A.M. (2011). The sensitivity and specificity of ultrasound for the diagnosis of carpal tunnel syndrome: A meta-analysis. Clinical Orthopedics and Related Research, 469(4), 1089-1094. The Skinny –The authors sought out to determine the sensitivity and specificity of ultrasound therapy for the diagnosis of carpal tunnel syndrome using…

Phantom Limb Pain, Residual Limb Pain, & Phantom Limb Sensation: Which is Which?
Written by Melissa Miller Introduction After amputation, the majority of individuals will experience phantom limb pain (PLP), residual limb pain (RLP), and/or phantom limb sensation (PLS). Experiencing these pains or sensations can greatly disrupt an individual’s quality of life. It is important to know what each of these are as each can impact the client…

Sign-up to Get Updates Straight to Your Inbox!
Sign up with us and we will send you regular blog posts on everything hand therapy, notices every time we upload new videos and tutorials, along with handout, protocols, and other useful information.
This is great! Keep them coming!
really interesting- thanks
We’re glad you liked it. We will keep them coming.
Love this!!! Thank you.
Glad you liked it!
Thanks for sharing !
What about PIP range of motion ?
Typically we instruct the patient with prom and to avoid active if it is causing the triggering to occur.
Thanks for sharing!
Important to know.
This is great – curious if there was a time frame of symptoms present for inclusion criteria and or for splinting to be effective? ie if the patient had triggering for less than 3 months splinting was found to be effective; or were patients who had symptoms for longer than x-amount of weeks/months were not included, etc etc? I have always been under the impression if symptoms are too severe/present for more than 4 weeks cortisone injection is kind of the gold standard as splinting is less effective at that point? Thank you!
Yes, the longer the condition goes on the more difficult it is to treat. From personal experience, I have had patients resolve their symptoms for trigger fingers that have been going on for 6 months