
Don’t Forget to Evaluate for Dorsal Scapular Nerve Entrapment
By Delaney Wright
If your patient presents with any upper thoracic pain, it is critical to take measures to evaluate for dorsal scapular nerve entrapment. In a study completed by Sultan et al. (2013), 55 patients with interscapular pain were evaluated clinically and via nerve conduction study and electromyography. While only 9 of the study’s participants were suspected of having dorsal scapular nerve entrapment, the authors found that 52.7% of the patients had electrophysiologic findings indicating this. Considering all the above information, when treating a client with upper to mid thoracic and interscapular pain, involvement of the dorsal scapular nerve should be considered a differential diagnosis and explored with further evaluation.
In the upper extremity setting, it is common for practitioners to treat their patients for a specific injury or diagnosis they were referred for but also treat other limitations or co-occurring impairments restricting function. During the treatment of primary injuries, a patient may also inform you about their pain in other areas, such as neck pain, back pain, or interscapular pain. Complaints of pain in any of these areas may point to a compression of the dorsal scapular nerve (Bishop and Varacallo, 2021; Muir, 2017). Because the dorsal scapular nerve is a motor nerve, it is often overlooked by practitioners and physicians when considering dorsal scapular nerve entrapment as a possible cause of pain in the upper thoracic region (Sultan & Younis El-Tantawi, 2013).

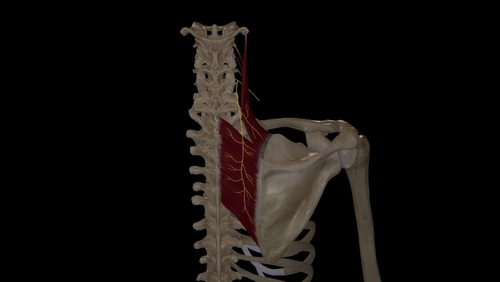
Dorsal scapular nerve neuropathy can present in the clinic in many forms, including pain, tightness, weakness, limited range of motion, dysesthesias, pruritis, scapular winging, and radiating pain along the posterolateral shoulder, arm, and forearm (Muir, 2017). The dorsal scapular nerve arises from the C5 nerve roots, passes posteroinferiorly through the middle scalene, then travels inferiorly between the posterior scalene and levator scapulae, taking an inferior route along the medial aspect of the scapula (Bishop and Varacallo, 2021). The dorsal scapular nerve provides motor innervation to levator scapulae, rhomboid major, and rhomboid minor, all of which are muscles contributing to the stability of the scapula (Bishop and Varacallo, 2021). The rhomboids work collectively to retract and downwardly rotate the scapula, while the levator scapulae contribute to scapular elevation and downward rotation (Muir, 2017).
One of the most common places described in the literature for entrapment of the dorsal scapular nerve is the middle scalene, often due to hypertrophy of this muscle (Muir, 2017). Additional dorsal scapular nerve injury mechanisms include repetitive lifting, compressive neuropraxia related to DME, repetitive overhead movements and overhead lifting, poor posture, and traction injuries to the nerve following automobile accidents (Muir, 2017). If, upon clinical review of a patient’s medical history and daily routine, you find that any of the movement mentioned above patterns or mechanisms of injury to the nerve may be likely, further evaluation of the dorsal scapular nerve may be warranted.
One way to evaluate dorsal scapular nerve neuropathy or impingement clinically is to observe the actions of these muscles; this can be done by asking the patient to retract their shoulders and/or elevate their shoulders while comparing bilaterally (Muir, 2017). Unilateral weakness when completing these motions may be a reason to suspect dorsal scapular nerve impingement/neuropathy. Additionally, decreased innervation of the rhomboids can lead to scapular winging, with the inferior angle of the scapula becoming more laterally displaced (Martin & Fish, 2008). This can be evaluated by having the patient complete shoulder extension from a fully flexed position (Martin & Fish, 2008).
Treatment for dorsal scapular nerve entrapment often consists of a conservative route with cervical spine stabilization, muscle relaxants, anti-inflammatories, activity modification, and therapy (Martin & Fish, 2008; Sultan et al., 2013). Therapy interventions often focus on trapezius strengthening to decrease the stretch placed on the rhomboids (Martin & Fish, 2008). Strengthening the trapezius also helps stabilize the shoulder girdle. The stability of the shoulder girdle facilitated by the muscles innervated by the dorsal scapular nerve is essential in the function of the upper extremity for various daily tasks. It is crucial to ensure that the accessory muscles that complete the exact motions of the rhomboids and levator scapulae are strengthened to reduce dysfunction and maintain a good scapulohumeral rhythm. Additionally, we can use manual therapy techniques such as soft tissue mobilization and gentle stretching of the middle scalene to decrease compression on this nerve (Skirven et al., 2021). If a conservative intervention route is unsuccessful, transection of the middle scalene may be considered when the nerve is compressed (Sultan et al., 2013).
As therapists, it is essential to evaluate all factors contributing to the limited performance of daily tasks. If your patient presents with any upper thoracic pain, it is critical to take measures to evaluate the dorsal scapular nerve. In a study completed by Sultan et al. (2013), 55 patients with interscapular pain were evaluated clinically and via nerve conduction study and electromyography. While only 9 of the study’s participants were suspected of having dorsal scapular nerve entrapment, the authors found that 52.7% of the patients had electrophysiologic findings indicating this. Considering all the above information, when treating a client with upper to mid thoracic and interscapular pain, involvement of the dorsal scapular nerve should be considered a differential diagnosis and explored with further evaluation.
References
Bishop, K. N., & Varacallo, M. (2022). Anatomy, Shoulder and Upper Limb, Dorsal Scapular Nerve. In StatPearls. StatPearls Publishing. http://www.ncbi.nlm.nih.gov/books/NBK459343/
Martin, R. M., & Fish, D. E. (2008). Scapular winging: Anatomical review, diagnosis, and treatments. Current Reviews in Musculoskeletal Medicine, 1(1), 1–11. https://doi.org/10.1007/s12178-007-9000-5
Muir, B. (2017). Dorsal scapular nerve neuropathy: A narrative review of the literature. The Journal of the Canadian Chiropractic Association, 61(2), 128–144.
Skirven, T. M., Osterman, A. L., Fedorczyk, J. M., Amadio, P. C., Feldscher, S. B., & Shin, E. K. (2021). Rehabilitation of the hand and upper extremity (7th ed.). Elsevier.
Sultan, H. E., & Younis El-Tantawi, G. A. (2013). Role of Dorsal Scapular Nerve Entrapment in Unilateral Interscapular Pain. Archives of Physical Medicine and Rehabilitation, 94(6), 1118–1125. https://doi.org/10.1016/j.apmr.2012.11.040
5 Comments
Leave a Comment
More To Read

Effectiveness of Conservative Therapy and Splinting for 1st CMC OA
Tsehaie, J., Sprekraijse, K., Wouters, R., Slijper, H., Feitz, R., Hovious, S., & Selles, R. (2018). Outcome of a Hand Orthosis and Hand Therapy for Carpometacarpal Osteoarthritis in Daily Practice: A Prospective Cohort Study. American Society for Surgery of the Hand, 1-11. The skinny: Non-surgical approaches (hand therapy & orthotics) are typically the go-to for…
Read More
Hand Therapy Article Review: The Radial Synergy Test, An Aid to Diagnose de Quervain’s Tenosynovitis
Chihua, L., Langford, P.N., Sullivan, G.E., Langford, M.A., Hogan, C.J., & Ruland, R.T. (2021) The radial synergy test: an aid to diagnose de Quervain’s tenosynovitis. HAND. epub ahead of print;1-6. doi: 10.1177/15589447211057297 Rapid Review By: Case Peters The Skinny: de Quervain’s tenosynovitis is a common pathology that involves swelling and thickening of the tendon sheaths…
Read More
Functional Home Exercises for Patients with Wrist Instability
Functional Home Exercises for Patients with Wrist Instability Ever wondered what brushing your teeth, dressing, making a U-turn, and playing sports have in common? They all rely on a stable wrist. Wrist stability is crucial for everyday activities, supporting wrist proprioception, coordination, motor control, stability, and mobility (Wietlisbach, 2019). For patients recovering from a wrist…
Read More
Sign-up to Get Updates Straight to Your Inbox!
Sign up with us and we will send you regular blog posts on everything hand therapy, notices every time we upload new videos and tutorials, along with handout, protocols, and other useful information.
I actually saw this once and managed to figure it out and fix it! Interesting stuff. Not all scapular winging is serratus anterior.
Good eye!
How do you properly regenerate this nerve? I’ve been injured for several years now.
Very helpful thanks for a new perspective.
finally find the root of my pain!!! been suffering from thoracic pain and scapular pain for years. numerous mri’s found nothing. i have relieved 90% of that pain massaging the scalene muscles.