
IFC vs TENS: Electrical Stimulation for Pain and Swelling
Filed under Treatments
In this article we’re looking at the difference between Inferential Current versus Transcutaneous Electric Nerve Stimulation (IFC vs TENS).
Transcutaneous Electric Nerve Stimulation (TENS)
TENS variations are often described by their technical characteristics: high frequency, low intensity (conventional TENS) or low frequency, high intensity (acupuncture-like TENS, AL-TENS) (Walsh et al., 2009).
How TENS Addresses Pain:
- Gate control theory, established in 1965, proposes a gate consisting of excitatory and inhibitory synapses that exist in the dorsal horn of the spinal cord (Walsh et al., 2009). This gate can regulate the amount of nociceptive traffic (painful stimuli) transmitted to the brain. This gate could be closed by non-noxious stimuli (e.g. touch, pressure and electrical currents), and block potential nociceptive stimuli.
- Increased release of endorphins through heat transmission, possibly more localized to the area of the pain
- Physiologically, conventional TENS selectively activates non-noxious low threshold afferent nerve fibers in the skin (Aβ-fibers). When administering TENS, Aβ nerve fiber activity is reported by the client to feel like a strong electrical paresthesia (pins and needles) beneath the electrodes (Walsh et al., 2009). AL-TENS is intended to generate a muscle twitch to activate small diameter afferent nerve fibers in muscles (Aδ) and descending pain inhibitory pathways. AL-TENS is administered at low frequency and high intensity currents over muscles, without pain.
Placement for TENS (Borst, n.d.)
- Can either be placed directly over the area of pain, or pads can “sandwich” the pain
- Pad placement effects the depth of the
current
- Close placement=superficial current
- Further placement= deep current
Inferential current (IFC)
Developed in the 1950s, IFC is most commonly used for pain relief (Kitchen, 2001). IFC is also claimed to reduce inflammation, and assist tissue repair (including bone fractures), and reeducate muscle (especially with incontinence).
How IFC Addresses Pain:
- IFC delivers current to deep-seated structures through an amplitude-modulated interference wave typically with the use of four electrodes (Kitchen, 2001).
- The wave is created by two out of phase currents that collide with each other to generate an interference with a frequency that can penetrate through the skin to deeper structures and even excite neurons.
- Use of IFC should generate a strong but comfortable electrical paranesthesia at the site of the pain, to generate Aβ activity (Kitchen, 2001).
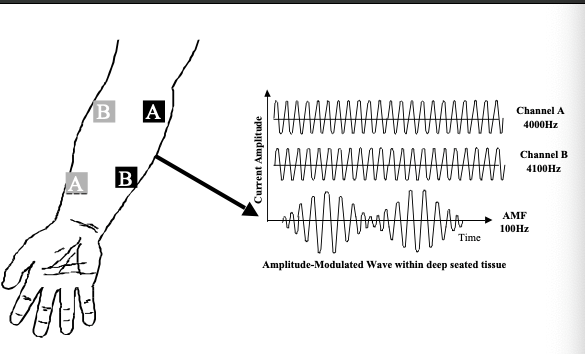
Image 1. Interference Wave (Kitchen, 2001)
Evidence to Support Use of Electrical Stimulation (TENS vs IFC) for Pain
- A Cochrane systematic review found preliminary evidence that TENS reduces pain intensity over and above that seen with no treatment for acute pain (Walsh et al., 2009). Definitive conclusions were limited by the high risk of bias, inadequate sample sizes, and unsuccessful blinding of treatment interventions. Although the use of TENS as a potential treatment option for managing acute pain is debatable based on these results, it can be self-administered, is safe, and can be inexpensive (Walsh et al., 2009).
- Current evidence suggests that overall TENS and IFC have similar effects on pain and improvements in functional outcome measures (de Almeida et al., 2018). There is a need for larger, well-designed and standardized studies to establish the best parameters for pain management due to limitations in current literature.
General Contraindications for Using Electric Stimulation: cardiac pacemakers (in areas close to device), near the carotid sinus, near, central venous and peripheral intravenous central catheter lines, metal implants, pregnancy, severe obesity, active bleeding, cancer, over the spine (Borst, n.d.)
General Precautions for Using Electric Stimulation: muscle fatigue, peripheral nerve pathology, cognitive impairment, allergic reactions, decreased sensation, open wounds, tendon or nerve repair surgery (need to wait 4-6 weeks typically to not displace tendon or nerve repair) (Borst, n.d.)
References
Borst, M. (n.d.). Test prep for the CHT exam (3rd ed.). American Society of Hand Therapist.
de Almeida, C. C., da Silva, V. Z. M., Júnior, G. C., Liebano, R. E., & Durigan, J. L. Q. (2018). Transcutaneous electrical nerve stimulation and interferential current demonstrate similar effects in relieving acute and chronic pain: a systematic review with meta-analysis. Brazilian journal of physical therapy, 22(5), 347-354.
Kitchen, S. (Ed.). (2001). Electrotherapy E-Book: evidence-based practice (11th ed.). Elsevier Health Sciences.
Snyder, A. R., Perotti, A. L., Lam, K. C., & Bay, R. C. (2010). The influence of high-voltage electrical stimulation on edema formation after acute injury: a systematic review. Journal of sport rehabilitation, 19(4), 436-451.
Walsh, D. M., Howe, T. E., Johnson, M. I., Moran, F., & Sluka, K. A. (2009). Transcutaneous electrical nerve stimulation for acute pain. Cochrane Database of Systematic Reviews, (2).
8 Comments
Leave a Comment
More To Read

Video-augmented mirror therapy for upper extremity rehabilitation after stroke
Kim, H., Kim, J., Jo, S., Lee, K., Kim, J., & Song, C. (2023). Video augmented mirror therapy for upper extremity rehabilitation after stroke: a randomized controlled trial. Journal of Neurology, 270(2), 831-842. Article Review: Shannon Skowbo The Skinny: This single-blind, randomized control trial aimed to assess the effects of mirror therapy for stroke patients…

Comparing Edema and Lymphedema: Understanding the Differences and Treatment Approaches in Hand Therapy
Comparing Edema and Lymphedema: Understanding the Differences and Treatment Approaches in Hand Therapy As hand therapists we often encounter patients presenting with swollen arms, hands, and/ or fingers, often attributing these symptoms to various conditions. Two commonly confused terms in this area are “edema” and “lymphedema.” While both involve swelling, they have distinct causes, presentations,…

5 return-to-cooking activities (that don’t require a kitchen)
Hand therapy can and should be very occupation-based. Every week, we hear comments from patients that back that statement up: “I need to get back to work” “I just want to golf again” “I can’t even open a water bottle” “My spouse has to do all of the cooking” Although standard exercises are helpful, it’s…

What is the real job of the Lumbricals?
Crowley, J. S., Meunier, M., Lieber, R. L., & Abrams, R. A. (2020). The Lumbricals Are Not the Workhorse of Digital Extension and Do Not Relax Their Own Antagonist. The Journal of Hand Surgery. The Skinny: What do the lumbricals do? There is a long-standing belief that the lumbricals act as a counterforce to the…

Sign-up to Get Updates Straight to Your Inbox!
Sign up with us and we will send you regular blog posts on everything hand therapy, notices every time we upload new videos and tutorials, along with handout, protocols, and other useful information.
Any pictures on how to position the inferential probes
You cross cross the electrodes. Requires four leads, leads are likely color coded with one set red and one set black or something similar. Place the first set of leads (red) across the area of desired treatment area so that it is diagonal like this / with one lead at each end point. Then place the other set (black) perpendicular to it like this \ again with one lead at each end. When your done you should basically have an X shape or your four leads dotted out like the corners of a box with alternating colors, red, black, red, black. This will make the current cross paths, reminds me of GhostBusters movie from the 80’s haha. Place the leads so that the current will flow across/through the area being treated. If the leads are too far apart the current may not connect to the other lead, if this occurs then place the leads closer until there is a current noted. Hope this was helpful. 🤗
Can you use just 2 electrodes for a small localized area (groin strain). Which method is recommended, IFC or TENS? My device also has the NMES option too.
I prefer IFC
it is suggested Not to use in Groin/sensitive & private areas.
hey, Scott if you have already tried it do let others know if there were any adverse effects or on the contrary any improvements. Cheers!
TENS should be used when only using one channel/color. You can also use both channels/colors if needed. With TENS you do not need to criss-cross the colors.
There is such thing as premod when using IFC. That allows you to run individual channels instead of in pairs.
Good point ! Thanks for sharing!