
A New Type of Median Nerve Glides for Carpal Tunnel Syndrome
Filed under Reviews, Uncategorized
Meng S, Reissig L.F., Beikircher R, Tzou C. H., Grisold W, Weninger W.J. (2015). Longitudinal gliding of the median nerve in the carpal tunnel: Ultrasound cadaveric evaluation of conventional and novel concepts of nerve mobilization. Archives of physical medicine and rehabilitation 96 (12). doi: 10.1016/j.apmr.2015.08.415.
By: Kyle Turcott
The Skinny
Carpal tunnel syndrome is a common neuropathy causing pain, weakness, and tingling in the hands and fingers. A frequently used conservative treatment for carpal tunnel syndrome includes nerve gliding exercises (median nerve glides). This is based on the assumption that an essential property of peripheral nerves is their ability to glide smoothly and that the lack of mobility leads to stress and neuropathy. There is much debate regarding the level of evidence and efficacy of nerve gliding to treat carpal tunnel syndrome. This article suggests that one reason there is insufficient evidence to support the efficacy of nerve gliding is that the current literature has primarily focused on median nerve movement proximal to the carpal tunnel. Using ultrasound scanning the researchers found that traditionally used nerve gliding exercises have a greater effect on the longitudinal movement of the median nerve proximal to the carpal tunnel and less effect on movement within the carpal tunnel. After collecting data on the findings, the researchers were unsatisfied with the results and created a nerve gliding exercise involving finger abduction and adduction.
In the Weeds
This study was broken into two parts. In the first part, researchers examined 9 upper extremities from fresh, nonembalmed whole-body cadavers (5 men, 4 women, median age 82 years). Bodies were initially examined using ultrasound to detect any anatomical anomalies. Using ultrasound guidance researchers implanted intraneural markers made of small wire along three sections of the median nerve. The first was within the carpal tunnel, the second was proximal to the carpal tunnel, and the third was between the two heads of the pronator teres. In addition, periosteal reference markers were placed into adjacent bones. After neural and periosteal markers were placed a physiotherapist simulated 6 movement traditionally believed to promote median nerve gliding (detailed below A-F). The image represents the exercises for the median nerve glides for carpal tunnel.
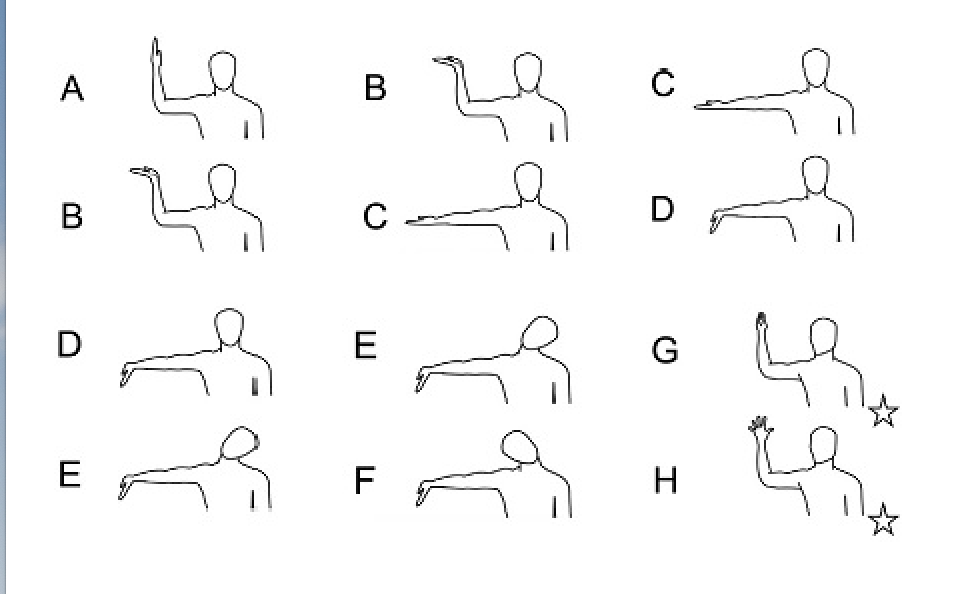
The 6 movements were broken up and reorganized as AB, BC, CD, DE, and EF and in each position the distance between the median nerve and the periosteal markers was recorded. The second part of the study was identical to the first part with the exception of an additional nerve gliding exercise GH which included finger adduction and abduction. Researchers found a statistically significant difference of median nerve movement within the carpal tunnel when comparing exercise GH with exercise A-G. In terms of distance, finger adduction to abduction was found to create 13.8mms of movement at the carpal tunnel. Wrist extension, elbow extension, and cervical contralateral and ipsilateral flexion were found to contribute 6.6mms of movement at the carpal tunnel. Movement proximal to the flexor retinaculum was similar (AG 12mm; GH 13.2mm respectively).
Bringing it Home
This research provides an interesting perspective on nerve gliding exercises and demonstrates improved distal nerve movement. This article helps to address the gap in the literature regarding median nerve movement within the carpal tunnel. The minimal invasiveness of this study is a strength as previous research into nerve mobility has been conducted on cadavers who have had significant alterations to normal anatomy. Cadavers are hardly a substitute for healthy live volunteers and the mean age of the sample did not reflect the typical age range of individuals struggling with carpal tunnel syndrome. The researchers noted this as an inherent weakness, however, due to the methodology it would have been impossible to conduct this study on live subjects. The article may not have an extraordinary impact on the current level of evidence and efficacy of nerve gliding treatment due to the fact that the axiom of the debate rests on the question, does lack of nerve mobility contribute to compression of the median nerve?
The research does provide promising evidence for a new nerve gliding exercise that promotes increased mobility of the median nerve at the site of concern. The exercise is also easy to teach and easy for patients to understand. In additional, it is one of the first studies to examine the longitudinal movement of the median nerve within the carpal tunnel. Continued research will be needed to assess the functional outcomes of patients who use the newly designed nerve gliding technique. If you would like to add this novel exercise into your nerve gliding repertoire see the images below for easy to follow instructions.
Step One: Begin with shoulder and elbow at roughly 90 degrees and digits adducted.

Step Two: Abduct Digits

Step Three: Adduct Digits

11 Comments
Leave a Comment
More To Read

Mirror therapy after a peripheral nerve repair in hand therapy
Rapid Review Paula, M. H., Barbosa, R. I., Marcolino, A. M., Elui, V. M., Rosén, B., & Fonseca, M. C. (2016). Early sensory re-education of the hand after a peripheral nerve repair based on mirror therapy: a randomized controlled trial. Brazilian journal of physical therapy, 20(1), 58–65. https://doi.org/10.1590/bjpt-rbf.2014.0130 The Skinny: Therapy is often provided following an…

Volkmann’s Contracture
Written by Melissa Miller Introduction Volkmann’s contracture is a rare condition that occurs after injury to the elbow and upper arm, typically from a crush injury. This condition can occur when acute compartment syndrome is left untreated. If unrecognized, Volkmann’s contracture can lead to a permanent deformity in the hand and forearm. Hand therapists are…

Article Review: Best Edema Management Techniques in Hand Therapy
Miller, L. K., Jerosch-Herold, C., & Shepstone, L. (2017). Effectiveness of edema management techniques for subacute hand edema: a systematic review. Journal of Hand Therapy, 30(4), 432-446. doi: http://dx.doi.org/10.1016/j.jht.2017.05.011 By: Ammie Ingwaldson The Skinny Edema is something therapists deal with on a daily basis and often is apart of most treatments. Managing edema can be a challenge…

Rotator Cuff Pain: K Tape + Rehab Short-Term Effects
Nguyen, T. N. A., Nguyen, N. H., Vu, D. K., & Cu, L. T. N. (2025). Short-term effects ofKinesiotaping combined with a rehabilitation program for rotator cuff-related shoulder pain: Arandomized, assessor-blinded clinical trial. Journal of Manual & Manipulative Therapy, 33(2),112–121. https://doi.org/10.1080/10669817.2024.2387913 The Skinny:The term rotator cuff related shoulder pain (RCRSP) encompasses a range of disordersassociated…

Sign-up to Get Updates Straight to Your Inbox!
Sign up with us and we will send you regular blog posts on everything hand therapy, notices every time we upload new videos and tutorials, along with handout, protocols, and other useful information.
This exercise is easy to teach and one that the patient will do vs the traditional ones.
Thanks for the article review! Very informative.
One way to really impact carpal tunnel symptoms is to do something that directly involves the carpal tunnel…like digit flexor tendon movement through the carpal tunnel. Unlike traditional median nerve glides, finger adduct/abduct requires movement of tendons through the tunnel. It’s astonishing how many interventions for carpal tunnel syndrome actually are more geared for a proximal etiology of distal symptoms.
And to echo Ms Rodriguez’ earlier comment, this exercise is easy to teach and do, and doesn’t require odd feeling (and looking) arm movements or positions. My patients are far more likely to stick with a regimen like this, than one where they need to refer to drawings for how to do the exercise, and that makes them feel awkward.
I totally agree!
Any protocol for reps etc?
I am OT in mental health but it is really interesting to know that ,even the exercise is easy
the image simplify the applying the exercise.
How many repetitions? Frequency? Any hold count. Such as: Hold 5 count each; 5 repetitions; 5x/day. I like the idea of it being simple yet effective.
Thank you!
Thank you for the explanation. I will try it! But, there is any evidence about nerve glinding in CST?
I have not found nerve gliding exercises to be helpful in my 30 years of practice. Often, I have seen where they have actually made this worse by patients over doing them. I have tried implement them multiple times thru the years.
Interesting. Thank you for sharing. They are commonly done in most settings. I think it might be time to take a dive into the literature and see if there are cases where it is not beneficials
Hi Tammy! I often find that the general tendon gliding found in most HEP/instructions are for higher level/less irritated nerves. So, once a patient starts with these they actually do get worse. At our clinic we start with nerve glides that target higher sensitivity. I believe the pages are found in Skirvens. We’ve had good success with these .