
Common Median Nerve Injuries
By: Madison Mott
Did you know!?
- Aside from the most common upper extremity nerve compression, carpal tunnel syndrome (CTS), there are several additional median nerve injuries.
| Pronator Syndrome Compression of the median nerve between the two heads of pronator teres. Result of recurrent, forceful gripping, forearm rotation, or elbow flexion. Signs include bothersome sensations when trying to rotate in supination and pronation | AIN Palsy Compression of the anterior interosseous branch of the median nerve. Identified by the inability to form the “OK” sign. Signs may be loss of motor control in the thumb, index, and middle fingers. | Lacertus Syndrome Compressed at the elbow, under the lacertus fibrosus. Can cause loss of feeling, strength, and dexterity. Signs may be difficulty handling small objects or having a tendency to easily drop objects. |
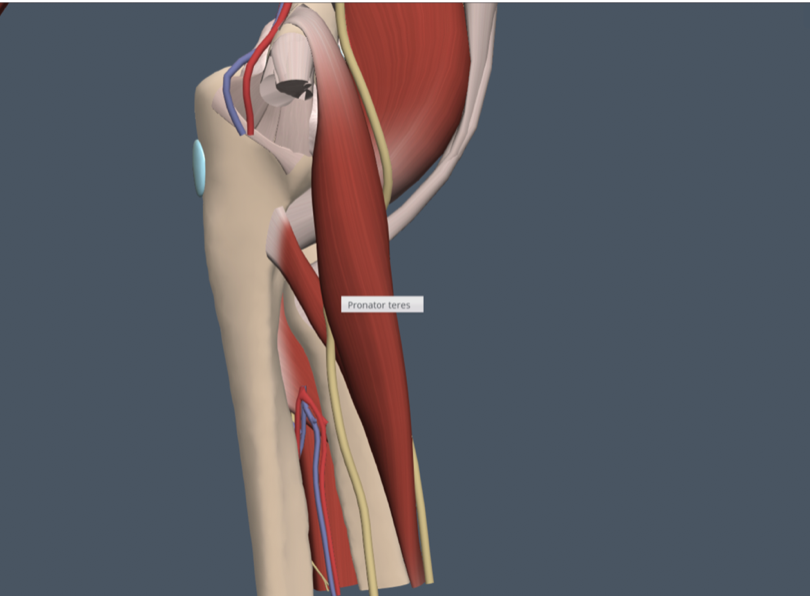
Pronator Syndrome
Anatomy:
Pronator syndrome occurs when the median nerve is compressed in the upper forearm as it passes along the elbow joint into the forearm compartment between the two heads of pronator teres. The median nerve begins in the upper arm and its branches extend into the fingers. When this nerve becomes entrapped at the elbow, a number of symptoms can present themselves. These are typically most noticeable and bothersome when trying to rotate the palms from facing upward to turning down towards the floor.
Pronator syndrome is often a result of recurrent, forceful gripping, forearm rotation, or elbow flexion, however, certain underlying conditions such as hypothyroidism and diabetes are considered risk factors as well. Common job roles that are especially prone to developing pronator syndrome include carpenters and mechanics. Athletes that participate in weightlifting, rowing, and those that use rackets are also at risk.
The presence of pronator syndrome can involve loss of sensation over the thenar eminence due to nerve compression. The Phalen maneuver and the Tinel sign are also often negative in pronator syndrome.
Conservative Treatment:
- Rest – decreasing overuse is crucial to recovery
- Elbow orthosis fabrication – should be worn 4-6 weeks
- Median nerve flossing
- Flexor stretching
- Myofascial release
- Kinesiotaping
Anterior Interosseous Neuropathy (AIN Palsy)
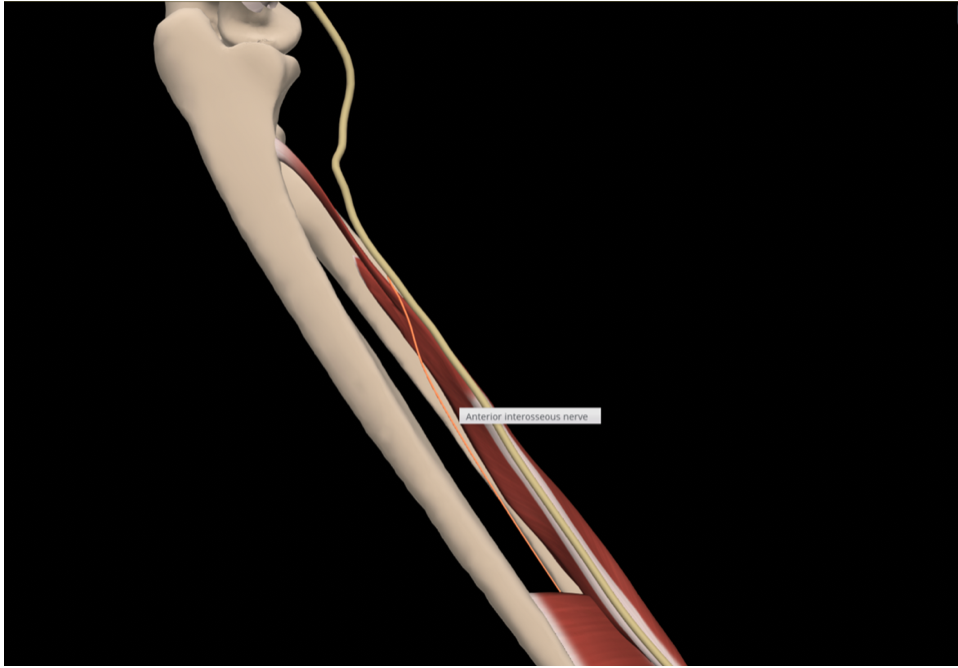
Anatomy:
The anterior interosseous branch of the median nerve is located at the elbow then moves into the anterior forearm. The anterior interosseous nerve innervates the flexor pollicis longus, pronator quadratus, and the deep flexors of digits two and three. There is no cutaneous branch, so neuropathy presents with muscle weakness and no sensory deficits.
On physical exam, this can appear by the patient being unable to touch the thumb to the index finger to make an “OK” sign. Another provocative test that could be performed is the pinch test where the patient will not be able to pinch a piece of paper with thumb and index finger. Certain activities such as buttoning a shirt, holding a pen, and grasping keys to turn on the car may be particularly difficult.
An injury to the anterior interosseous nerve most commonly occurs with complex trauma, whereas an isolated injury is rare. Specifically, AIN is most commonly reported following fractures and crush injuries.
Conservative Treatment:
- The exact protocol for AIN treatment remains unclear. It has been reported as being
due to inflammation or compression, therefore, surgeons recommend surgical decompression or waiting for spontaneous recovery within 3-12 months.
Lacertus Syndrome
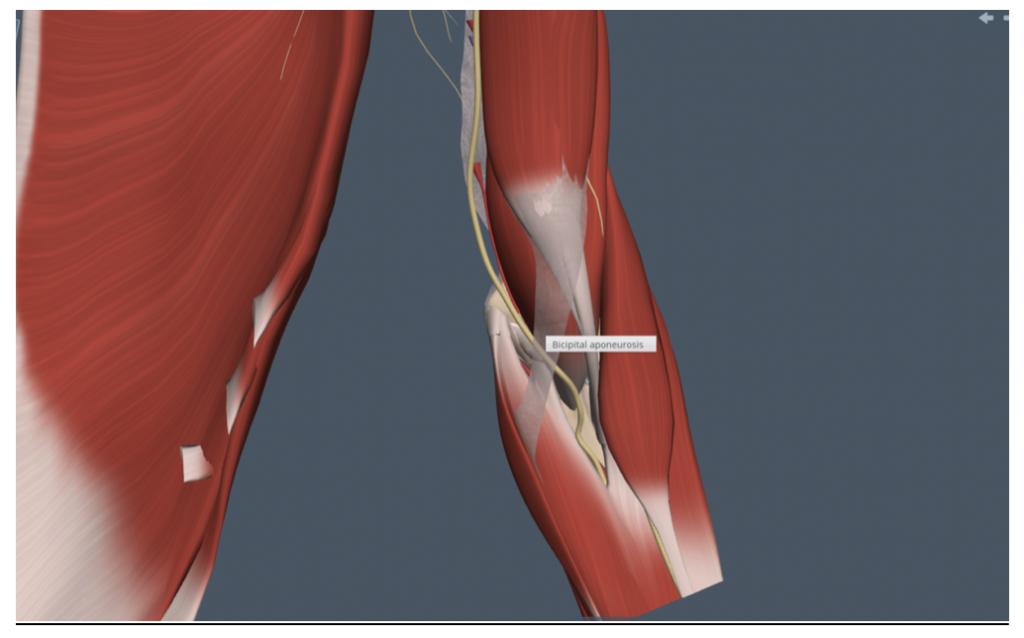
Anatomy:
Lacertus syndrome occurs when the median nerve becomes compressed at the elbow.
Specifically, it becomes entrapped under a fibrous expansion called lacertus fibrosus, which runs obliquely from the tendon of the biceps to the inner side of the elbow. The manifestations of lacertus syndrome are both sensory and motor. It causes numbness and pain in the forearm that can radiate to the elbow, as well as loss of feeling, strength and dexterity. The patient often has difficulty handling small objects and may have a tendency to easily drop objects. Lacertus syndrome affects both men and women, typically after 35 years of age. Manual work, overwork, and repetition of movements with the forearm in pronation are risk factors.
Conservative Treatment:
- The exact protocol for lacertus syndrome treatment remains unclear. Conservative treatment would be similar to that of pronator syndrome.
References
Anterior interosseous nerve syndrome. In Touch Hand Therapy. (2020). Retrieved February 9, 2022, from https://www.intouchhandtherapy.co.nz/our-blog/anterior-interosseous-nerve-syndrome
Dydyk, A. M., Cascella, M., Sarwan, G., & Negrete, G. (2021, November 27). Median nerve injury. StatPearls [Internet]. Retrieved February 1, 2022, from https://www.ncbi.nlm.nih.gov/books/NBK553109/
Lalonde, D. (2015, May 19). Lacertus syndrome: A commonly missed and misdiagnosed median nerve entrapment syndrome. BMC Proceedings. Retrieved February 9, 2022, from https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4445778/
Median nerve: what is it, anatomy, function & common Conditions. Cleveland Clinic. (n.d.). Retrieved February 1, 2022, from https://my.clevelandclinic.org/health/body/21889-median-nerve
2 Comments
Leave a Comment
More To Read

Effectiveness of Conservative Therapy and Splinting for 1st CMC OA
Tsehaie, J., Sprekraijse, K., Wouters, R., Slijper, H., Feitz, R., Hovious, S., & Selles, R. (2018). Outcome of a Hand Orthosis and Hand Therapy for Carpometacarpal Osteoarthritis in Daily Practice: A Prospective Cohort Study. American Society for Surgery of the Hand, 1-11. The skinny: Non-surgical approaches (hand therapy & orthotics) are typically the go-to for…

Creating an Action Plan for Addressing Mental Health in the Clinic
Blog By: Rachel Reed As hand therapists, our care for our patients must be driven by the goal of treating the whole person, not just their hand or injury (Hannah, 2011). Occupational therapy is a unique profession in which we are equipped to view our patients through a holistic lens. With this lens, we are…
")
Carpal Tunnel Treatment: Splinting Only vs Splinting & Conservative Treatment
Short-term clinical outcome of orthosis alone vs combination of orthosis, nerve, and tendon gliding exercises and ultrasound therapy for treatment of carpal tunnel syndrome. Sim, Sze En et al. Journal of Hand Therapy, Volume 32, Issue 4, 411 – 416 The Skinny- Carpal tunnel syndrome (CTS) is the most common compression neuropathy. Compression of the…

Top 5 DIP Flexion Exercises
By: Tori Rhodes Lately, we’ve had a handful of patients roll through our clinic with pretty significant limitations to DIP flexion. So, we’ve collected a selection of go-to exercises for these individuals. We’ve included a few of those here. From cat bites and fracture sites to mallet fingers and skin grafts, many individuals who are…

Sign-up to Get Updates Straight to Your Inbox!
Sign up with us and we will send you regular blog posts on everything hand therapy, notices every time we upload new videos and tutorials, along with handout, protocols, and other useful information.
Hello, my name is Emily and I am a hand therapist in the Austin area with 27 years of clinical experience. I find that I often get patients with a diagnosis of carpal tunnel syndrome who display symptoms of median nerve compression elsewhere in the upper extremity, such as pronator teres syndrome. I have found that dry needling is an effective treatment for these patients (Vas et al., 2017). I was wondering if you could share some of the relevant research that you have found on dry needling as an effective treatment modality?
Hi Emily, Thank you for sharing. I was briefly able to look at the article you suggested. It looks like it would be a good one for an article review. We have a few months lined up in the queue but could potentially do this one in the future. Thanks for sharing.